An Opte Project visualization of routing paths through a portion of the Internet. (http://creativecommons.org/licenses/by/2.5) via Wikimedia Commons.
Sadly, one of the most common cyberattacks is upon health care centers, particularly ransom-ware attacks upon hospitals. While digital records and telemedicine are proving essential during the COVID-19 pandemic, hospitals’ reliance upon digital resources also make our health care systems vulnerable to attack. As this article by Jocelinn Kang and Tom Uren says, cyber-defense efforts now need to prioritize our health care systems.
If you are interested in hearing more about global topics, please listen to my podcast, Dispatch 7. You can find it on Spotify here, or by searching whichever podcast platform you prefer.
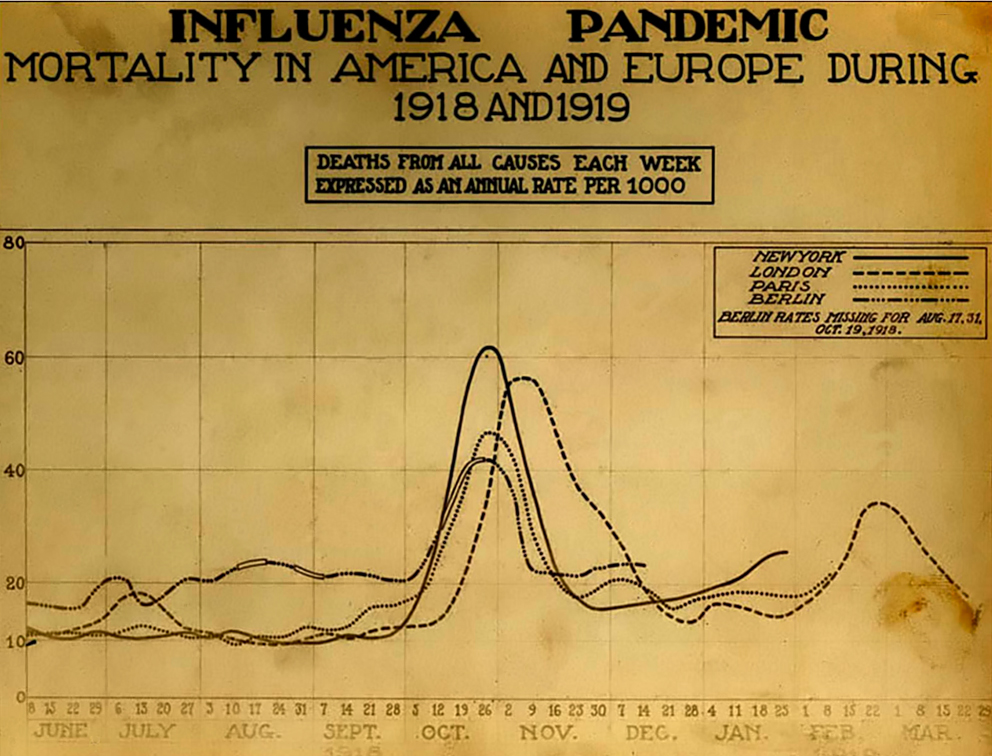
The Spanish Influenza. Chart showing mortality from the 1918 influenza pandemic in the US and Europe. Wikipedia commons.
The New York Times had a remarkable story yesterday morning by Donald G. McNeil Jr. , which talked about a company (Kinsa) that markets smart thermometers. The company can use the data on fevers from these devices to foretell where the outbreak will grow, before that data shows up in other sources. You can see the company’s map here. As the NYT article says, there is so much interesting data here.
As someone who has spent a lot of time in Florida (my mother was a mystery writer, who set her novels in the bars of West Florida) I am deeply worried by the data on southeast Florida, as well as around Tampa. And even some of northern Florida, such as Duval county, has high levels of atypical fevers. But what is happening in Michigan? The map around Detroit has not lit up as red as Miami, but there is a swath in the south of the state where the levels of atypical fevers have raised. The swatch stretches as far west in the state as Kent county. I wouldn’t have expected what appears to be happening in Utah county, and Salt Lake county, Utah. But these counties still do not light up as much as Broward, Palm Beach, and Miami-Dade do in Florida. …
Image of globe on light, McGill University. Photo by Smallman
In our textbook, the health chapter begins by this comparison of nations: “Chile, Costa Rica, Cyprus, Guadalupe, Hong Kong, Israel, Macau, Malta, Martinique, Singapore, and the United Arab Emirates are a diverse set of nations and territories. Yet they all have one fact in common: their citizens live longer than those of the United States, as do the citizens of many developed countries (United Nations 2006). This truth is unexpected, given the wide gap between the wealth, power, and technology of these countries and that of the United States. But health inevitably becomes linked to broader issues of politics and policy.” This is certainly the case in the United States’ ability to respond to a pandemic.
What have some of the lessons of this pandemic been for the United States? Our health care system has a number of weaknesses during an epidemic:
A health care system that invests heavily in technology, but less so in people, such as the public health professionals who do contact tracing.
A lack of recent experience with pandemics, such as South Korea and Canada had with SARS and MERS.
An inadequate stockpile of personal protective equipment. A failed effort to develop a stockpile of ventilators wasted over a decade, and left the United States undersupplied.
A popular belief that epidemics are something that happens elsewhere, so that the first and best response is only to put in place border restrictions.
A sense of hubris, so that outbreaks in China or South Korea are assumed to be something that could not happen here, because our hospitals -with their advanced technologies- would be able to manage the situation.
A health care system in which peoples’ insurance is tied to their employment. This has meant that when people lose their employment during a pandemic, they also lose health care.
Deep health inequalities, which mean that case fatality rates may vary widely depending upon class and geography.
A lack of sick leave for U.S. workers, so that people feel compelled to come to work when they are sick, or to face an immediate financial crisis if they are forced to stay at home.
A sense of hubris regarding the U.S. medical system, which led U.S. health authorities to reject a German developed test for COVID-19 that the World Health Organization (WHO) endorsed. Instead, the U.S. frittered away precious time developing its own test. When that did not work, the CDC and FDA wasted even more time resolving the situation.
A CDC and FDA that had become too swamped by bureaucracy and hence struggled to adapt, despite having outstanding and dedicated people. The system’s senior leadership has ossified.
A U.S. health care system that is too decentralized to respond to a national level emergency, although this decentralization also has some benefits when there are failures at the top.
An over-reliance on overseas manufacturing for key health goods, for everything from masks to medications.
A society that undervalues the very people who turn out to be particularly critical during a pandemic: janitors, grocery store clerks, truck drivers, nurses, farmers, and others. As many people have said, it is only during a pandemic you learn whose job really counts. And there is not a good correlation between peoples’ pay and how important their job truly is. The same holds true for respect.
A high rate of chronic diseases that leave people vulnerable to a disease such as COVID-19. The “diseases of development” such as diabetes, sleep apnea, high blood pressure and morbid obesity have led to higher case fatality rates. Most of these issues connect to the Standard American Diet (SAD) and the U.S. food system. No technology can replace a good diet.
A chronic underfunding of public health. A good public health system is like a seat belt. You forget that it should be there until you really need it. And it seems kind of basic, but when the moment comes, there is nothing else that can replace it.
Basic public health relies on people, and salaries are expensive. But not having an adequately funded public health system is what is truly expensive. Contact tracing, outreach, education, follow-up, monitoring, epidemiology, and health communication take time and people. Perhaps because they do not rely as much on technology they are also undervalued in the United States, which always likes to use technology to solve all problems. But there is no substitute for public health professionals.
The basic systems that are always there in public health -nurses in schools, communication campaigns, testing systems, contract tracing- are the same systems that are needed in a pandemic. So having good public health in ordinary times gives you the tools and the people that are needed during extraordinary times.
Local market sign in Cambridge, Massachusetts, March 17, 2020
The COVID19 pandemic is now moving quickly. While northern Italy has been overwhelmed by infections, Spain and Iran are also now experiencing a disaster. Here in the United States, there are serious outbreaks in Seattle and New York. So what are the best maps and other data visualizations to keep track of what is happening? Here are my top recommendations:
Outbreakinfo is an outstanding dashboard, which provides a vast amount of information in a limited space. This is one of the top three sources for tracking the pandemic.
The Worldometer Coronavirus webpage has a plethora of charts with data on the outbreak, in particular country by country data on infections, new infections, deaths and recoveries.
Health map provides another global map of the outbreak, although it is not accompanied by the data in charts that accompanies the John Hopkins’ map above. It does have, however, an “animate spread” feature that shows a visual history of the virus’s spread, which is hypnotic.
I am very grateful to Jim P. for this guest blog post.
One Expat’s Life In China In The Time Of Corona Virus
A PSU Alum’s observations
A few things to get out of the way up front. I moved to China after graduating from PSU in the summer of 2015, and getting my Type Z (Foreign Expert) visa which took a few months. I finally arrived here in late December of 2015. I live and work in the city of Yantai, on the northeast coast of the peninsula portion of Shandong Province. The city has a population of ~7 million, though it feels much smaller than Portland because it is spread out over a much larger area, and there are large swaths of agriculture (namely corn) between different areas of the city.
When the Corona virus was first announced, I was getting off work before the beginning of the two week long Spring Festival holiday (which is what most English people think of as “Chinese New Year”). The next day, I came down with a cold. Nothing like having a nasty cough when everyone is freaked out by a disease that’s major symptom is a cough (I didn’t have a fever, or flu-like symptoms). At first it seemed like most things were still open, and much like life as usual for the beginning of the holiday (except everyone had masks on). However, as soon as the fireworks were over, everybody went back inside, and ventured out rarely (mostly to take out trash). …
Today seems to be the day in which the words and numbers that international organizations and national governments used to describe the COVID-19 pandemic increasingly diverged from facts. To begin there was an overall context in which the virus rapidly spread in the Middle East, while cases dramatically climbed in Korea (833). In the Middle East, there were new cases in Afghanistan, Bahrain, Egypt, Iraq, Israel, Lebanon, and the United Arab Emirates. Most of these cases were tied to Iranian travelers. In Italy the number of cases rose sharply. Venice ended the remaining days of Carnival. Italians in northern Italy rushed to stores, some of which were cleaned out and left with empty shelves. In the United States, ongoing problems with testing for SARs-CoV-2 has meant that health authorities have been unable to test at scale, as in Korea, Singapore and Canada. Finally, in China the rate of increase has slowed, but the nation still has over 77,000 cases. But neither the rising number of cases nor other problems caused corresponding expressions of concern by WHO or the Iranian government.
First, Dr. Tedros at the World Health Organization (WHO) said at a press conference that the WHO would not call COVID-19 a pandemic. Indeed, the WHO has stated that it no longer uses “pandemic” as a category. At the current time, there is ongoing transmission of a novel virus in multiple world regions, with a case fatality rate of perhaps two percent. If this is not a pandemic, what would be? The goal of deleting the term pandemic seemed to be more to avoid causing fear than to accurately describe reality. If the WHO does not play the role of declaring a pandemic, then who does? The risk of this is that the public in different nations may begin to lose confidence in the WHO. The pandemic exists even if the category does not. …
This letter written by Mi Fei. By 米芾(べい ふつ、1051年 – 1107年、中国の北宋末の文学者・書家・画家) [Public domain], via Wikimedia CommonsI am very grateful to our guest blogger, who teaches at a university in China, for this powerful guest blog post:
January 24th is the biggest holiday of the year in China: the lunar Chinese New Year. As usual, most Chinese prepared for it several weeks before the occasion: food, candies, tickets back home…Nobody expected this New Year would become a most unforgettable one even in his/her whole life. The coronavirus became a household word almost overnight and quarantine also came suddenly before people realized. Over the past almost a month, people, especially those in epidemic areas, went through hard times. On the other hand, we are moved by one story after another about the devoted doctors, nurses, volunteers and all those in the whole world that extended their hands to help.
The spring term in our university originally planned to start on February 17. At the end of January, it was clear that the starting date had to be postponed. The school administration sent some documents early in February notifying all the staff and faculty to make a plan for the month. We were asked to make better use of the online platforms and resources. As a result of the encouragement from the Ministry of Education and development of online courses, there have been thousands of moocs available on the Internet for free, which in my opinion cover nearly all disciplines. As for my course (college English), we have been utilizing the online platforms for the textbook developed by the publishing press over the past five years. Therefore, what we need is to transfer the platforms from kind of self-learning to more guided learning. At the same time, we selected some relevant moocs either as a required component of the course or as recommended resources. …
Canadian health authorities have announced a positive test for SARS-2-COV in a returning traveler from Iran. Yesterday, Iranian authorities announced two deaths from COVID-19. There are eighteen confirmed cases, which are spread across the country, and include a case in Tehran. It would seem plausible based on a the death count so far, and a case fatality rate of two percent, that there are over a hundred cases circulating in Iran. It is telling that one of the Iranian cases is a doctor, which suggests transmission within the health care system. Given that a case has appeared in Canada, which likely has fewer travelers than Iran’s neighbors such as Iraq, we can expect that health authorities will announce new cases in these nations in coming days. Unfortunately, two of Iran’s neighbors -Afghanistan and Syria- are in the midst of civil wars, and have damaged health care systems. Sadly, the cases in these countries will likely first be detected in critical cases, which will make it unlikely that these countries can control community transmission. …
I am grateful to Celine Kuang for the following guest post:
Studied at Shanghai University, August – December 2019
Studied at Southwest Minzu University, January 2020
I’m a double major student in international studies and Mandarin Chinese. I mainly went to China to study the Chinese language and gain a broader cultural experience. I studied at Shanghai University for five months before going to Southwest Minzu University in Chengdu, China. During school breaks, I traveled around China to explore its cities, including Beijing, Nanjing, Hangzhou, Xi’an, Guangzhou, Shenzhen, Zhuhai, Shaoxing, Suzhou, and more. Everywhere I went China emphasized its status of being the most populated country in the world. The virus changed all of China’s populous and vibrant cities to ghost towns within a week’s time. In December is when the virus first started to appear. The Chinese government thought the news would create fear amongst its citizens, so they restricted news of the outbreak. The government was right about fear and as a result, many rumors started going around on social media. One Chinese friend even asked me if the U.S. planted the novel coronavirus outbreak. I was shocked that someone would ask me that, but I answered that it’s not possible. That was only the beginning of a whirlwind of issues.
During Chinese New Year many Chinese migrate back to their parent’s home to celebrate which helped to spread the virus even faster than anticipated. Less than a week into the family gathering, the Chinese government started locking down cities, increasing health checks in neighborhoods, and restricting all forms of travel between cities everywhere. This caused serious traffic congestions and delayed resources from efficiently reaching consumers. I’m not suggesting that China shouldn’t take such drastic measures, but these measures do have economic consequences as many scholars and researchers have already explained. Yet, even more concerning may be the how the necessary resources such as medical face masks (to prevent the virus from spreading) are becoming extraordinarily rare in this short time period. Many people are unable to buy new masks. Some pharmacies even started selling face masks at ten times the original price to seek profit at another’s expense. Some people started to create and sell their own brands of face masks but the quality of the masks is so poor that it can be considered a scam for the less educated populations. My mom informed me of her friend asking if she would buy face masks from the U.S. and send the masks internationally to them. Soon after, the friend told my mom not to bother sending the masks because no packages right now can be received anyway due to travel restrictions all over China. The friend is hoping that steaming and boiling them under hot water would help disinfect the used the masks so the family may continue using them.
I, myself, barely made it out of China during this hectic time. Three days into the Chinese New Year break, the Chengdu program I was in said they’ll continue classes and we’ll all wear masks during lectures. The following day they said they will consider holding lectures through webinars. That next morning I woke up to a classmate knocking on my bedroom door asking for my Chinese visa extension receipt. She told me the assistant resident director will be going to the consulate to get the passports of several others and mine back from the Chinese Consulate. She said I should check the conversation going on in the group chats and that the program is now cancelled. I was dumbfounded that in such a short period of time every changed for the worse. I emailed my scholarship and said I need to return to the U.S. as my program is being cancelled and the heightened travel advisory went from level one to level four in a week’s time. That night I bought plane tickets to leave Chengdu. Besides me there are hundreds of other students on the same scholarship as I am. Two days after receiving numerous emails(including mine), the scholarship sent a mass email out telling us to leave ASAP. We must all leave within eight days they told us.
Every time I read the news it says how many flights are being cancelled between China and the rest of the world. I finally packed everything I needed to leave but one days before my flight it got cancelled. I became worried. I called my airline through an international call for forty minutes to change my tickets. Plane tickets went from around 400 USD to 1000 USD in two days. That’s when I realized the vulnerable situation I was in. I was lucky enough to make it out of China before being infected. To be certain I still went through the fourteen day self-quarantine after I returned to the U.S.
Many Chinese friends have posted on the popular messaging app of China, WeChat, that they hope school would start soon or they can’t stay indoors any longer. Some of them went out for the first time after weeks of quarantine at home with their family. They posted photos of deserted parks, streets, and metro stations. Some posted food they ordered from the few restaurants that are still open during this novel coronavirus outbreak. It is understandable why China is trying to protect the non-exposed population by restricting travel between cities. However, the problem of being able to provide the necessary resources, such as face masks, to citizens throughout China can really hinder the control of the virus. This is only one of numerous issues following that China and the rest of the world has to worry about. In three months’ time the death rate is over 2,100 (this does not include those who died at home without going to the hospital) which is nearly three times the death rate of SARS. Of course, there is the hope that the virus will be controlled sooner rather than later. Currently, over 16,000 have recovered from the virus but how many more will die before the situation is under control? I hope the worse will pass by soon for everyone in China and a cure will emerge for the infected.
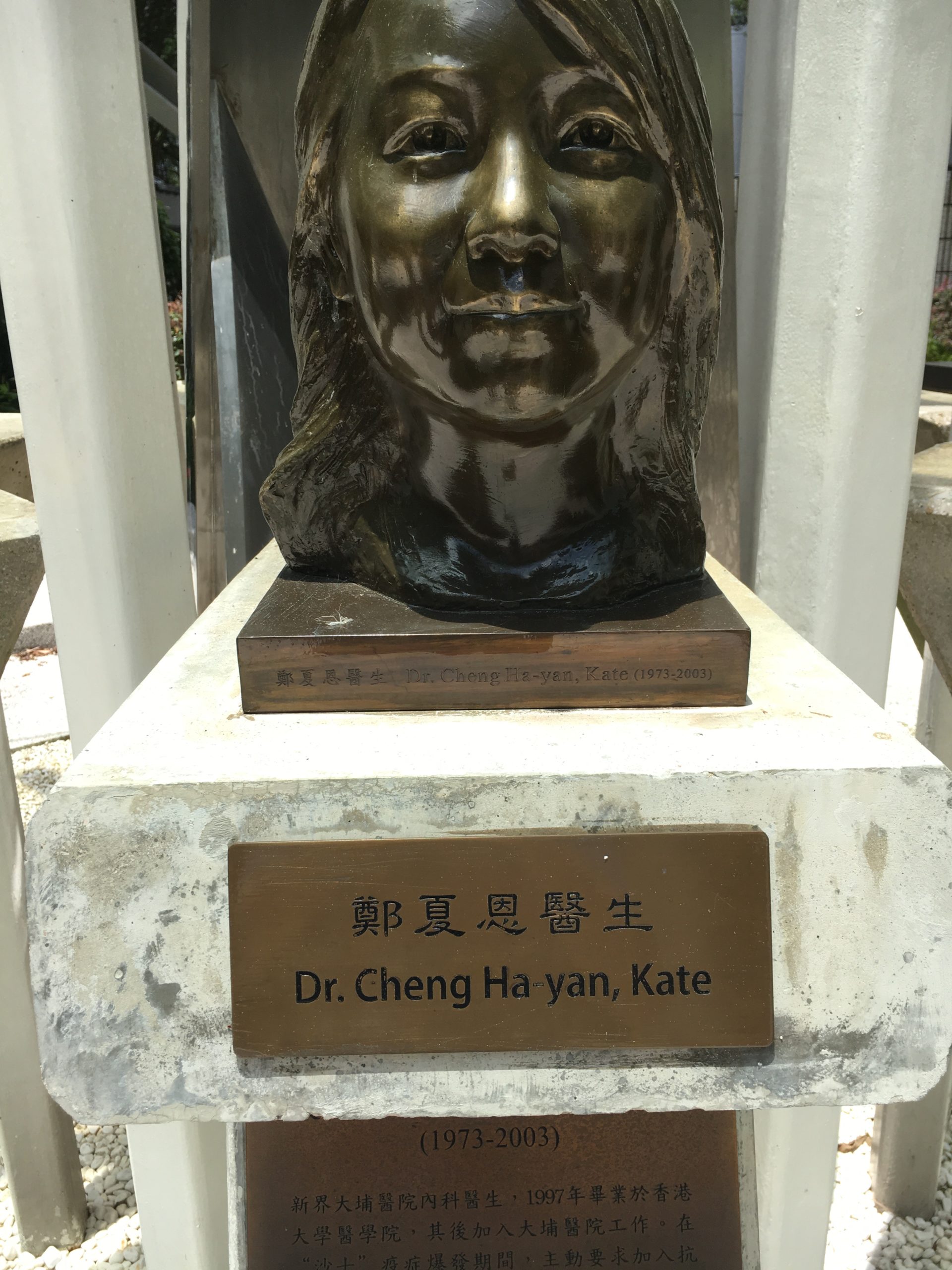
Bust and Plaque at the Fighting SARS memorial, Hong Kong
It is time for a hard discussion in the field of global health. In an earlier blog post I talked about how quarantine saved American Samoa during the 1918 influenza pandemic, whereas Western Samoa (now Samoa) lost nearly a quarter of its population. In the latter case, a single ship from New Zealand named the Tahune brought the virus. This video, “1918 Samoa & The Talune – Ship of Death” on YouTube shows the impact that this single ship had on the island’s history. At that time decisions about quarantine and trade were not made by the island’s inhabitants themselves, but rather by colonial administrators. Similarly, in Labrador the Moravian supply ship Harmony brought the 1918 influenza to Indigenous communities, which destroyed some entire population centers. You can see the human cost of this experience in the video, “The Last Days of Okak,” which Newfoundland archives has placed on YouTube.
The point with these two examples is that neither of communities that were affected had any say in the travel restrictions that could have protected them. Those decisions were made elsewhere. In American Samoa a harsh quarantine saved people. Of course there were economic costs to the quarantine, but those were ephemeral, whereas the lost lives in Western Samoa were permanent. But there is another lesson to the experience of these islands. The case fatality rate for the 1918 influenza was perhaps two percent globally. But there were communities (such as in Alaska) where the fatality rate was drastically higher. Some populations are more vulnerable than others, based on isolation, poor health care facilities, economic deprivation, lack of sufficient living space, and other factors. As in 1918, we may see drastic differences in fatality rates with COVID-19. …