For the last twenty years or more I have been doing work on public health. A key part of that work has been studying conspiracy theories during pandemics. I first started working on this topic when I was doing research on HIV/AIDS in Latin America. While I spent time in Brazil, Cuba and Mexico, I heard many conspiracy theories about HIV/AIDS: it was designed in a US military lab to control populations in developing countries or that pharmaceutical companies had found a cure that they kept secret to ensure their profits from HIV treatments. Upon returning home I heard a great deal of HIV denialism -the belief that AIDS was not caused by a virus- in my classes from my students. It’s hard to believe now, but twenty years ago there were many students who would argue passionately that HIV was caused by drugs or pesticides sold by Monsanto.
In the years that have followed I have written about the conspiracy theories that have surrounded everything from Zika to the 2009 influenza pandemic. What has always struck me about these conspiracy theories is how much recycling they entail. The same narratives are reused no matter the new health threat that emerges. Sometimes I think that I have worked on this topic for too long, and that I am at risk of repeating my own arguments. But these theories matter. Why would a pregnant women in a Zika affected area put on insect repellent if she doesn’t believe that the vector is a mosquito?
Ebola is a classic example of the damage these theories can cause. I have a new paper out that asks why there was such a difference in how social media companies responded to conspiracy theories about Ebola and COVID. It’s a brief essay but I hope that it will provoke some discussion.
Shawn Smallman, 2023
Smallman S. Conspiracy Theories and Ebola: Lessons Learned Important for Future Pandemics. Norton Healthcare Medical Journal. 2023; 1(1). doi:10.59541/001c.77445
Early in the pandemic I thought it likely that COVID-19 would have multiple waves, perhaps three like the 1918 influenza pandemic. So I never thought that the pandemic would end quickly. But over the last six or seven months I keep finding myself thinking that this time, finally, it must be ending. In June I had both of my COVID-19 vaccinations, cases in the US were plummeting, and I thought that by this winter it would have finally ended. Then Delta arrived, and filled the emergency rooms of the US south. This fall I was able to travel to Lisbon, where I am carrying out historical research on the 1918 influenza pandemic. When I arrived this October Portugal was the most vaccinated country in Europe, and was the subject of a front page article in the New York Times. And yet since I’ve arrived I’ve seen the case right rise dramatically. Not long ago I was looking at the New York Times country data page, and saw that cases in Portugal had increased 116% in two weeks. The country’s case rate may pass that of the US before long. Keep in mind that not only does Portugal have a high vaccination rate, but also people are very good about wearing masks here. It’s common to even see people wearing them in the street, at least if the street is crowded.
While Portugal is facing serious challenges, the situation is far better here than it is in other places, such as Austria. The COVID-19 incidence there is growing at a stunning rate. The government is implementing firm measures, but is facing mass protests. Other countries, such as the Netherlands, are in the same situation, as we have seen from the protests in Rotterdam. Still, the situation is much worse in Eastern Europe, where in some countries such as Bulgaria only a quarter of adults are vaccinated.
It’s in this context that we are receiving news about a new -as yet unnamed- variant in South Africa. There is a lot that we don’t know about this variant yet. The German news channel recently interviewed one expert who suggested that it might be 500 percent more infectious than Delta, although he stressed that we just don’t know yet. Even such qualified statements are dangerous. We will have more data soon. Still, there is a lot of speculation that this variant might partially evade vaccines, because there are so many mutations, including a number involving the virus’s spike protein.
Nations are rushing to block flights from South Africa. Britain was very slow to respond to the Delta variant, and allowed travel to continue for weeks after it was clear that Delta might lead to a new wave. But after the news of this new variant emerged Britain blocked air travel from Southern Africa. Many other nations are also imposing travel restrictions. Of course, this variant has already been found in Israel. And in Hong Kong -where it was brought by a traveler from South Africa- it managed to spread to one other person in a quarantine hotel. Blocking travel from South Africa will help to buy some time, which might be put to use gathering data on the virus. It might also give people the time to be fully vaccinated and get their boosters, if they are in countries in which vaccines are readily available. But in the end, it won’t be enough. Without a complete border and air travel shut down, a highly infectious virus will certainly spread globally.
Given that Delta is already so severe in Europe, the timing for the emergence of this variant could not be worse for this region as it heads into winter. People are exhausted from the pandemic. But it’s not over. Please, if you are not vaccinated, hurry to be vaccinated now, so that your body has time to build immunity. While all medical treatments have risks, the risks of COVID-19 are much greater, billions of people have had the vaccines, and a new variant is coming. And if you are eligible for a booster, now would also be a good moment for that too. Two months ago there was a significant debate around whether boosters were necessary. Given what’s happening now in places like Portugal, there’s no doubt that only focusing on the severity of cases, and not on transmission, is a poor public health approach.
Let’s hope that this proves to be a false alarm, and that the new variant doesn’t greatly increase severity, transmission, or vaccine evasion. We all deserve some luck.
On October 6, 2021 the World Health Organization made a historic announcement. They had approved the world’s first malaria vaccine, which had been in development for more than thirty years. Of course, this amount of time is trivial compared to the history of malaria itself. The disease is one of humanity’s oldest scourges. There are tombs along the Nile that hold mummies who died of malaria. As Rome collapsed in the late fourth and fifth century malaria ravaged Italy, and depopulated entire regions. When a Spanish conquistador descended the Amazon river from Peru to the Atlantic, the friar Carvajal reported that the river bank was so densely settled that each town lay only a crossbow shot from the next one. A hundred years later these communities had vanished. And even today in Africa and southeast Asia every year hundreds of thousands of children either die or are left with life long disabilities (such as epilepsy) from the disease. In many regions, it’s almost impossible to avoid, although the WHO has put great effort into promoting sleeping nets and insecticides.
I recently did a podcast interview with Dr. Marylynn Steckley, who talked about her experience researching in Haiti, while both she and her family suffered from frequent illness. Malaria makes some parts of the world difficult to live and work in for everyone, including outsiders. Although I have not had malaria, I have known many people who have, and for whom it had an enduring impact on their health. Indeed, for many of my Africanist colleagues it was almost assumed that they would acquire the disease, and perhaps live with it’s long term effects. Some of my African colleagues -such as one archaeologist- have many stories about their bouts with the disease.
It’s ironic that during this terrible COVID-19 pandemic we finally have some positive news. This is not only the first vaccine against malaria, but -as many observers note- the first against any parasitic disease. As such, it’s a proof of principle. Some people have wondered if it might prove to be impossible to develop vaccines against these class of diseases, since parasites have evolved to overcome the human immune system for long periods of time. Now we have seen that it can be done.
The vaccine is known as RTS,S/AS01, and it has its limitations. It’s only effective around 40% of the time. It also requires four doses. Even so, given that more 200 million people a year are infected with malaria, this can prevent an immense amount of suffering. More vaccines are in the development process.
There is something remarkable about this new vaccine. It relies on an ingredient from an evergreen tree (the quillay tree) that grows in only one place in the world, Chile on the Pacific coast of South America. This rare ingredient is an adjuvant, which is an ingredient in a vaccine that helps to create an immune response in the human body. The first useful medication for malaria was quinine, which comes from a tree grown in the Amazonian region. Now, once again, Indigenous knowledge and a South American plant, is proving vital in the struggle against malaria. It also places intense pressure upon the stocks of the quillay trees, especially as this ingredient is also being used to develop at least one COVID-19 vaccine and a shingles vaccination. There is currently a technological race on to understand how to extract this ingredient from seeds and immature Quillay trees, because currently the supply replies upon mature trees of at least thirty years of age.
Humanity still has a long way to go in this fight against a killer that even affected pharaohs. But -with help from an usual Latin American tree- the world has its first vaccine, and that is an immense step forward.
In my latest podcast episode for Dispatch 7, I talk about what we’ve learned from the COVID-19 pandemic. Why did some developed countries respond more poorly than developing nations? What lessons does history teach us about the value of quarantine? And what is a One World approach to global health?
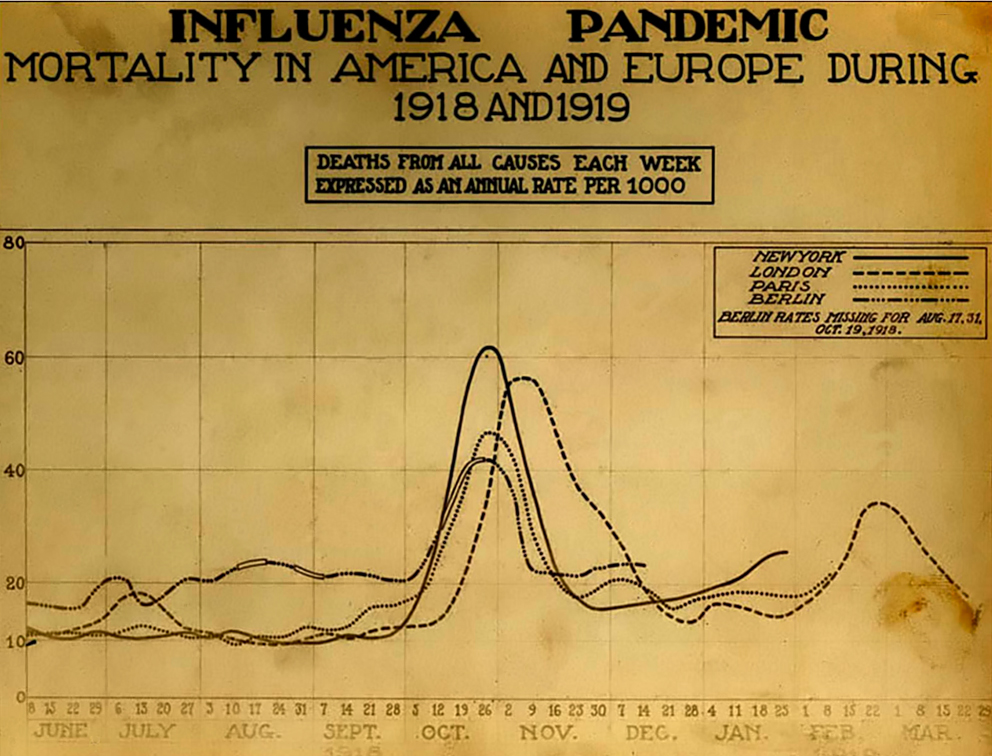
The Spanish Influenza. Chart showing mortality from the 1918 influenza pandemic in the US and Europe. Wikipedia commons.
According to the CDC, as of September 10, 2021, 652,480 Americans had died of COVID-19. This is nearly as many as the perhaps 675,000 Americans who died in the 1918 flu pandemic. But there seems to be much less fear of COVID-19 now than there was of the influenza pandemic then, at least in some parts of the United States. Why?
Of course, the first point to make is that there was certainly denial and minimizing in the United States in 1918, which people used to justify holding everything from war-bond rallies to weddings. Still, after the terrible month of November 1918 this declined. Is the difference between then and now in part that we live in social media bubbles? I think that there is some truth to this, but there are a few factors that explain the different attitude that many people had towards influenza then.
In 1918, there was a “W” shaped mortality curve, as most people who died were infants, young adults and the elderly. Before the arrival of the delta variant, there was a perception that those people most at risk of COVID-19 were over 65, and perhaps their deaths were less shocking. In contrast, younger people felt relatively safe. In 1918 it was people in the prime of their life who were dying, as well as their children. This made people feel more vulnerable.
Today, people typically die in the hospital. In 1918, if you lived in a rural area -as did most of the population- a trip to the hospital would take time and might not be easy. More people were cared for –and died– at home. I think that this meant that people saw the results of outbreak much more directly. Today, the ill vanish into hospitals. Their suffering leaves nurses and doctors traumatized, but isn’t visible in the same way that the 1918 pandemic was, when family members and neighbors would see the bodies taken out the front door.
There were three distinct waves to the 1918 influenza pandemic. But the fall 1918 wave had a much higher peak in the death rate. Of course, the spring 1918 influenza outbreak was terrible in some places such as the military camps in Kansas. But by November 1918 the number of deaths was so crushing that denial was no longer an option in many communities. People were too busy taking care of their neighbors; everyone could watch the gravediggers. COVID-19 has been more spread out, which has changed how people have talked about it.
The US population was much smaller in 1918 than now, at just over 103 million people, versus 328.2 million. So although the total numbers of deaths are similar, the death rate was roughly three times higher a century ago. People saw much more death during the 1918 pandemic.
I also wonder if people didn’t have a different attitude towards medicine. The 1918 pandemic took place before most childhood vaccines, antibiotics, and modern therapies. People had more limited expectations for what a doctor might do. Now, it might be that many people expect that if they go to the hospital they will be saved, because they have often seen sick family members or friends healed in a hospital. I can’t prove this, but I suspect some COVID-19 patients are shocked when they find out that they will die. In 1918, people respected and valued doctors, but the life expectancy for men was 36.6 years, and 42.2 for women. People didn’t feel as invulnerable -and didn’t assume that the hospital would save them- because they were more familiar with death. In 1917 -the year before the pandemic- the second most common cause of death in the US was pneumonia and influenza.
Of course, in 1918 people relied heavily on newspapers and the government for information, whereas now people turn to social media. But I think that people were more familiar with infectious illness in 1918, and experienced the pandemic in a different way than with COVID-19. This difference perhaps helps to explain why in many states people seem to be much less afraid of COVID-19 than their great-grandparents were during the 1918 pandemic.
Shawn Smallman
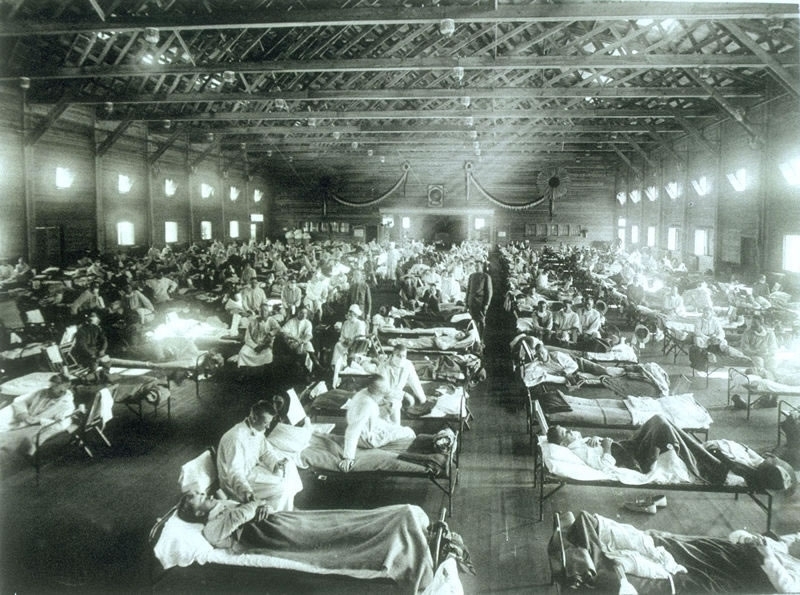
Historical photo of the 1918 Spanish influenza ward at Camp Funston, Kansas, showing the many patients ill with the flu- U.S. Army photographer
Few countries have done such a good job controlling COVID-19 as Australia, but now the nation is facing a significant test in Bondi. A driver (sometimes described as a bus driver, and sometimes as a “car-for-hire driver) worked shuttling air crews to quarantine hotels, as well as driving the general public. Even though he was a front-line worker, he was not vaccinated. He also seems to have had poor personal protective equipment (PPE). Unfortunately he was infected with COVID-19. While in the contagious phase he went to see a movie, visited a cafe twice, had lunch at a Japanese restaurant, and drove a large number of passengers.
What was most remarkable, however, was his visit to a mall in Bondi (Westfield Bondi Junction). In that mall, he appears to have infected people despite “fleeting contact” which was recorded on store cameras. There were a number of such cases. One woman was sitting outside at a cafe, where he was sitting indoors. Normally the risk of outdoor transmission is believed to be low. But she was infected. In another case he appears to have passed a shopper, in the briefest of interactions, which was captured on CCT cameras. But that person was infected. The old rules -fifteen minutes of contact is required for transmission; outdoor transmission is rare- don’t seem to apply in this case, which is causing some justified worry in Australia. People are lining up in their cars for testing.
Fortunately, people seem to have been isolating as asked, and wearing masks. As of today, there are still only eleven cases. Hopefully, this outbreak will be controlled. Health authorities are currently dealing with over a hundred exposure sites. One of the places people were exposed was on a bus. This incident raises this question: is the unusual pattern of spread the result of the new, more transmissible Delta variant, or was this something particular to this individual patient. Epidemiologists are discussing this question is multiple venues. Currently 3.2% of Australians are fully vaccinated.
Whatever the answer in this case, we may see more examples. As was the case with Taiwan, the critical failing was around quarantine hotels and air crews. All people who work in any respect with air crews (in nations without community transmission) need to be fully vaccinated. And the system for hotel quarantine needs to be improved. And more broadly, here in the US we are still far off our record for one day COVID-19 vaccinations, despite a slight uptick recently. People need to be vaccinated now, as the Delta variant is growing rapidly. Although it was originally thought that it would be the dominant strain of COVID-19 in the US as early as this August, it’s now looking as though that might happen as early this July. If you’re fully vaccinated, you have a good level of protection and don’t need to worry. If you’re not fully vaccinated, now is the time to do so.
Throughout the last several months, the US Center for Disease Control has messaged that in order to catch COVID-19 you had to be within six feet of an infected person for fifteen minutes. This was reassuring information. But sadly the US was also perhaps in a difficult place to answer detailed questions about COVID cases, because the contact tracing system has been overwhelmed. The US has also lacked a national COVID tracking app, as many other nations (Australia) have had. Realistically, this would have been a political impossibility to implement in the US, given that even masks have been highly politicized here. So, how realistic was the CDC’s guidance?
In Korea, contact tracing has been highly effective. It turns out that the combination of a digital tracking app with highly skilled contact tracers has been more successful than either purely digital or human tracing would be. And what Korea has learned -in a remarkable piece of scientific work- is that in one case a high school senior was infected after five minutes of exposure and from twenty feet away. The infection took place in a restaurant (which had video recording) and it turns out that an air conditioning unit was wafting air from an infected person towards the student. The quality of the data that the contact tracers obtained -and the history of how they learned it- is remarkable, and well worth reading.
There is nothing magic that happens at the six feet mark from another person. And being exposed to an infected person indoors can be risky even when the CDC’s old guidelines might make us feel safe. In this case, Korea has given us not only important information, but also let us see the quality of information contact tracing can provide. The key message is that neither six feet of distance, or avoiding more than fifteen minutes of exposure to another person, may be enough to keep you safe from infection, particularly indoors. So indoor dining is probably always unsafe.
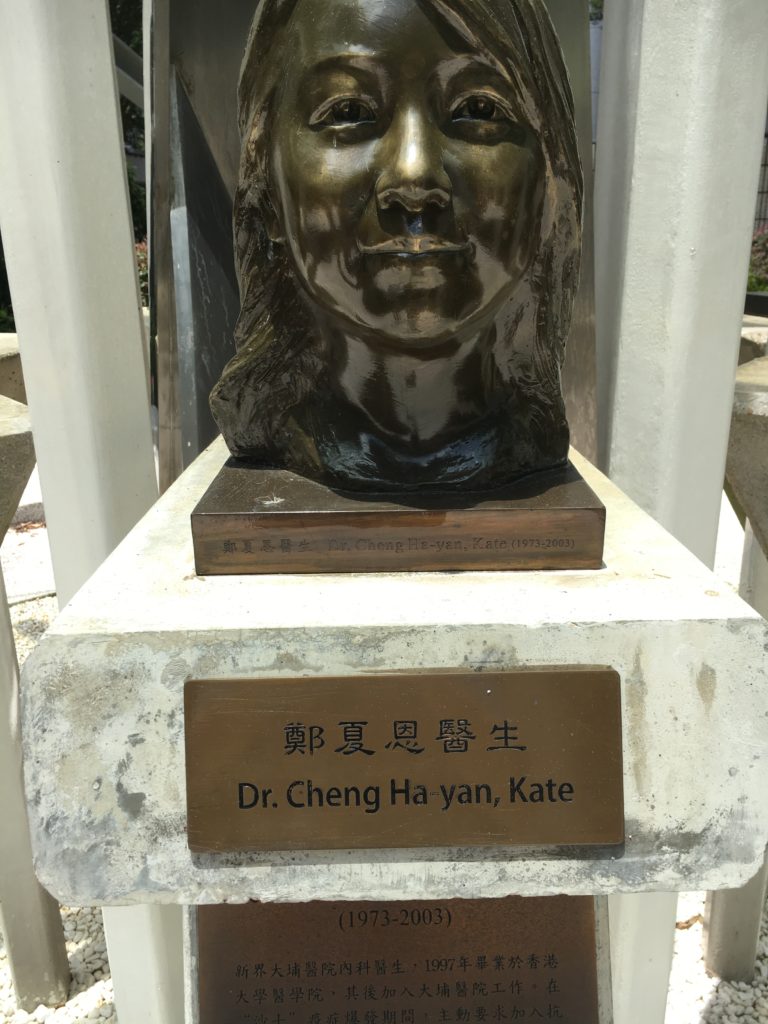
Bust and Plaque at the Fighting SARS memorial, Hong Kong
A recent study published in the American Journal of Microbiology journal, MBIO, suggests that MMR 2 vaccine helps to prevent COVID-19 symptoms. It’s a study based on a small population (80), but the MMR blood titers show a very strong association with the severity of COVID-19 illness. People with high titers were all asymptomatic. Everyone who became severely ill had titers under 32. This wasn’t the first article exploring this idea of an association between MMR vaccination and COVID-19 resistance. But it’s an intriguing one that deserves more attention and research.
As a press release from the American Journal of Microbiology states, this could also explain why children don’t seem to get seriously ill. The MMR blood titers fall as you age. And the elderly may never have had this vaccine, in part because they’ve had measles or mumps. One significant point to the study was that having had the mumps doesn’t protect you. People need to have the vaccine itself. This contradicts the argument of vaccine critics who say that it’s better to have natural immunity. But in this case, the vaccine seems to give better immunity. As someone who had mumps as a child (and then gave it to my sister) I’m in favor of a vaccine-based approach to public health, rather than natural or herd-immunity.
I want to emphasize again that this study was based on the MMR blood titer results of only eighty people who had COVID-19. So this is a preliminary study. But the risks of the MMR are very low; at least hundreds of millions of people have had it since it was first introduced in 1971. Please note that this study only examined the MMR 2, not the quad vax, which also includes varicella.
Even though new COVID vaccines are coming soon, it will take months to roll the out at scale. It would be wonderful if we could use an existing vaccine with a long track record for safety to help us to buy time.
Historical photo of the 1918 Spanish influenza ward at Camp Funston, Kansas, showing the many patients ill with the flu- U.S. Army photographer
After the wonderful histories of Alfred Crosby and John Barry, readers might wonder if there is truly anything new left to write about the 1918 influenza pandemic, which killed between 50 and 100 million people world-wide, at a time when the world’s population was much smaller. Laura Spinney’s detailed, beautifully written and insightful work shows how much study can yet be done on this topic.
As Spinney describes in the opening to her book, in the 1990s much of the writing on this pandemic had been done on Europe and the United States. Of course there were exceptions. In Canada Eileen Pettigrew created a rich narrative of people’s experiences from survivors accounts, while Betty O’Keefe and Ian MacDonald told the story of how medical officer Fred Underhill fought the disease in Vancouver, Canada. There were similar accounts of popular experiences with the pandemic in other countries, such as Australia and New Zealand. But voices in Asia, Latin America and Africa were often not included. Since the 1990s there has been a plethora of work in many different nations, at the same that scientific advances have made it possible to have a much better understanding of the pandemic.
Spinney’s history takes full advantage of this study. She also has a gift for seizing upon the lives of individuals to tell a broader story, whether it was a young man in Rio de Janeiro, Brazil or a scientist in Republican China. She weaves together these narratives to create an overarching view that is truly global. After reading the work I find myself curious to learn more details on individuals, such as a woman affected by the pandemic in South Africa, who then created a religious (and perhaps millenarian) movement.
While such individual accounts are powerful, I particularly like chapter fifteen, in which she described how the same virus had dramatically distinct impacts in different places. Why would the same disease cause mortality rates in excess of 80 percent in some remote Alaskan and Labradoran villages, and far lower rates elsewhere? Of course, the flu was not unique in this respect. I wrote an entire book trying to understand the diversity of HIV epidemics in Latin America. What is perhaps most striking to me is that after a century of earnest study, many of these questions remain unanswered.
What is clear was that the pandemic utterly devastated some locations. In Western Samoa, twenty-two percent of the population died. In the Pacific, on the island of Vanuatu perhaps 20 languages died because of the heavy mortality that the virus brought. Given Brazil’s catastrophic response to the COVID-19 pandemic, and the disproportionate impact that the virus is having on Brazil’s Indigenous peoples, might something similar happen in the Amazon rain forest now? As Spinney states, there was a strange paradox to the virus. Cities often saw high mortality rates, but isolation caused terrible vulnerabilities in remote communities.
What was also striking to me was her discussion of the influenza’s aftermath. In part, this was reflected in such societal trends as a loss of faith in science. Will we be struck by a similar trend with COVID-19? But there was also a physical legacy of the virus, as many people suffered either psychological trauma over the loss of loved ones, or debilitating physical effects that lingered long after the virus was gone. Of these, perhaps the most famous was encephalitis lethargica. While it cannot be proven that the 1918 influenza pandemic caused this disorder -again so much remains unknown about this tragedy- the onset of the one was accompanied by the emergence of the other, as some people remained paralyzed -but apparently aware- for decades. Will COVID-19 have similar health effects that linger for more than a generation? The thought is chilling, given that one recent pre-publication from Korea just reported that up to 90 percent of COVID-19 survivors still report symptoms months later.
Still, what most struck me is that we are now having the same debates now that we had over a century ago: “One 2007 study showed that public health measures such as banning mass gatherings and imposing the wearing of masks collectively cut the death toll in some American cities by up to 50 percent (the US was much better at imposing such measures than Europe).” While now it is the US struggling to persuade its citizenry to wear masks, there is a haunting quality to the debates from this time. Some challenges that faced public health authorities then echo during the COVID-19 pandemic now, although (as far as I know) the death threats and public vilification of public health leaders was uncommon in America a century ago. So perhaps things have gotten worse. Spinney’s last two chapters are remarkably prescient for a book that was published in 2018.
I’ve spend much of the last twenty years working on public policy and infectious disease, first with my book on HIV/AIDS, and more recently with Zika and avian influenza. Some factors are constant, such as the fact that conspiracy theories emerge with every pandemic. One of the most common human urges when faced with an outbreak is to find someone to blame. But what depresses me is that I don’t think the historical studies or public policy achievements make much difference in the long run. In 2018 I published an article on wet markets in Hong Kong, which recommended that the special administrative region consider closing them. Of course, COVID-19 did not emerge in Hong Kong, but likely from a wet market in eastern China. One of the reasons that I hate conspiracy theories is that the distract from the real actions that could make people safer. They also make pandemics and outbreaks seem mysterious and unpredictable.
In fact, people have been studying coronaviruses in China since SARS emerged in 2003 precisely because such an event might take place. This was entirely predictable. As I said in an earlier blog post, how much human suffering might have been avoided if China’s wild game markets -which particularly cater to an older and wealthier clientele- had been closed. Yet even the Chinese government -with all its power and influence- either would not or could not do this. And now social media accounts spread tales that this outbreak is caused by 5G, and people in Britain burn cell towers. Two million people have died globally and winter is drawing closer in the northern hemisphere. We all know what happened in November 1918. Now we must now hope that a different virus will have a dissimilar impact.
Yet behind the scenes scientists have laid the groundwork that will allow for vaccines to be more quickly developed, because much basic science work has been completed. For all the frustration with sciences’ failures and limitations, the hope that we have now doesn’t come from conspiracy narratives -which don’t lead to any constructive steps- but from the often ignored work by nearly anonymous scientists in global laboratories. This work lacks the drama of the conspiracy theories, but the time-consuming and methodical study has laid the groundwork for the greatest vaccine push in human history. Conspiracy theories are easy to create. Real public policy or scientific advances are far more difficult, time-consuming and (often) difficult to understand. Spinney’s work is built upon a detailed examination of both the historical and scientific literature that has been built up over the last century, particularly the last twenty years.
It has long gone out of fashion in academia to look for lessons or a moral in history. But if this line of thinking is taken too far, it might lead people to question the value of history entirely. If historical study cannot give us lessons for the present period, isn’t it little more than a hobby for the affluent few? Laura Spinney’s brilliant book shows how a careful understanding of history can provide us the context to better understand current challenges. Sadly, in this current moment, it’s probably difficult to interest people in reading a work about a past outbreak. Spinney’s magisterial, carefully researched and beautifully written book deserves a broad audience. Highly recommended.
References
Spinney, Laura. Pale Rider : The Spanish Flu of 1918 and How It Changed the World. First US Trade Paperback ed. New York: PublicAffairs, 2018.
See also the following works for more reading on this topic.
Barry, John M. The Great Influenza : The Epic Story of the Deadliest Plague in History. New York: Viking, 2004.
Crosby, Alfred W. America’s Forgotten Pandemic. West Nyack: Cambridge University Press, 2003.
Canadian popular histories:
O’Keefe, Betty, and Ian Macdonald. Dr. Fred and the Spanish lady: Fighting the killer flu. Heritage House Publishing Co, 2004. (Full disclosure: this press also published my history of an evil spirit in Algonquian belief. Please note that I have no control over the price of physical copies of this book on Amazon, which sometimes surges to hundreds of dollars for mysterious reasons. So if you click on this link for my book, please don’t send me unhappy emails to complain about the book’s price).
Pettigrew, Eileen The silent enemy: Canada and the deadly flu of 1918. Saskatoon: Western Producer Prairie Books, 1983.
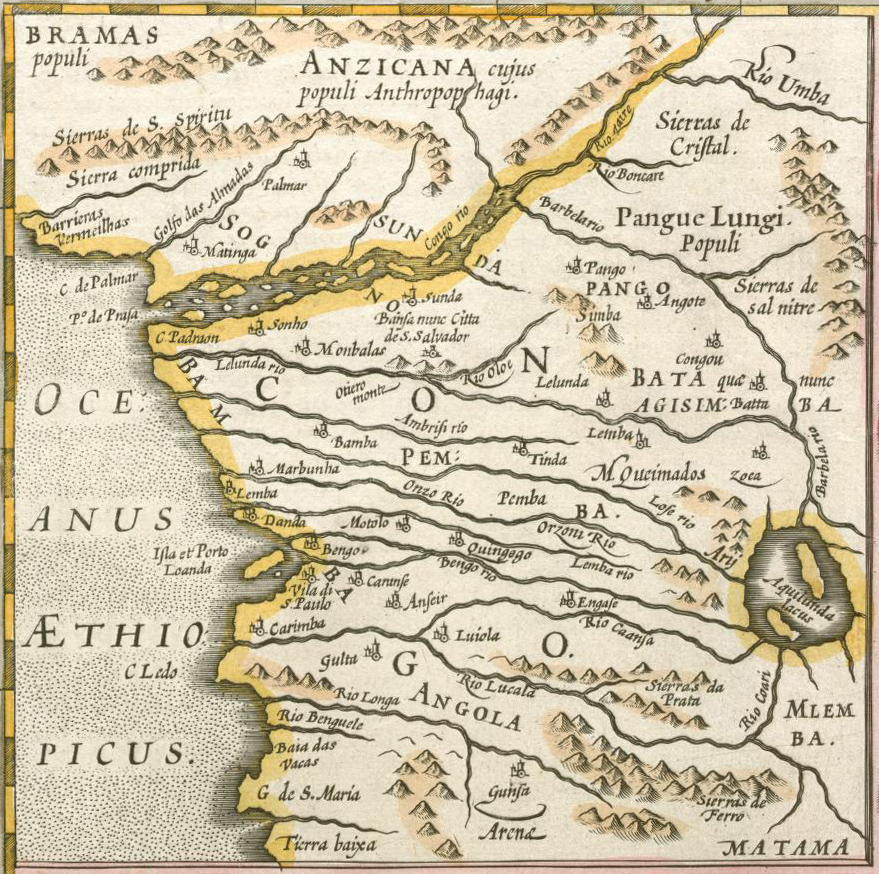
Mercator Map of the Congo, 1595, from the Northwestern University Library Maps of Africa collection, accessed through Wikipedia.
I wrote a book, the AIDS Pandemic in Latin America, and have studied public policy and infectious disease for nearly twenty years. Here is a lecture that I wrote (around 2010?) for an “Introduction to International Studies” class. It would need to be updated now; it may also some references to my own experiences, which would need to be removed. But my hope is that it might prove a useful starting place for someone who wants to do a lecture on this topic in a similar class.