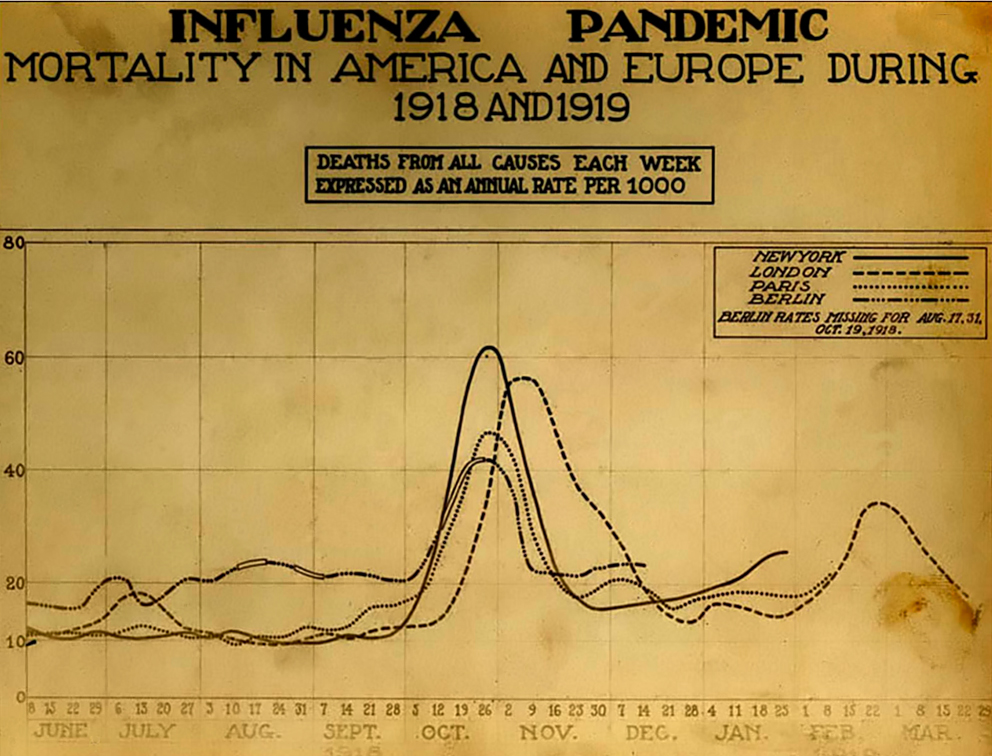
The Spanish Influenza. Chart showing mortality from the 1918 influenza pandemic in the US and Europe. Wikipedia commons.
According to the CDC, as of September 10, 2021, 652,480 Americans had died of COVID-19. This is nearly as many as the perhaps 675,000 Americans who died in the 1918 flu pandemic. But there seems to be much less fear of COVID-19 now than there was of the influenza pandemic then, at least in some parts of the United States. Why?
Of course, the first point to make is that there was certainly denial and minimizing in the United States in 1918, which people used to justify holding everything from war-bond rallies to weddings. Still, after the terrible month of November 1918 this declined. Is the difference between then and now in part that we live in social media bubbles? I think that there is some truth to this, but there are a few factors that explain the different attitude that many people had towards influenza then.
In 1918, there was a “W” shaped mortality curve, as most people who died were infants, young adults and the elderly. Before the arrival of the delta variant, there was a perception that those people most at risk of COVID-19 were over 65, and perhaps their deaths were less shocking. In contrast, younger people felt relatively safe. In 1918 it was people in the prime of their life who were dying, as well as their children. This made people feel more vulnerable.
Today, people typically die in the hospital. In 1918, if you lived in a rural area -as did most of the population- a trip to the hospital would take time and might not be easy. More people were cared for –and died– at home. I think that this meant that people saw the results of outbreak much more directly. Today, the ill vanish into hospitals. Their suffering leaves nurses and doctors traumatized, but isn’t visible in the same way that the 1918 pandemic was, when family members and neighbors would see the bodies taken out the front door.
There were three distinct waves to the 1918 influenza pandemic. But the fall 1918 wave had a much higher peak in the death rate. Of course, the spring 1918 influenza outbreak was terrible in some places such as the military camps in Kansas. But by November 1918 the number of deaths was so crushing that denial was no longer an option in many communities. People were too busy taking care of their neighbors; everyone could watch the gravediggers. COVID-19 has been more spread out, which has changed how people have talked about it.
The US population was much smaller in 1918 than now, at just over 103 million people, versus 328.2 million. So although the total numbers of deaths are similar, the death rate was roughly three times higher a century ago. People saw much more death during the 1918 pandemic.
I also wonder if people didn’t have a different attitude towards medicine. The 1918 pandemic took place before most childhood vaccines, antibiotics, and modern therapies. People had more limited expectations for what a doctor might do. Now, it might be that many people expect that if they go to the hospital they will be saved, because they have often seen sick family members or friends healed in a hospital. I can’t prove this, but I suspect some COVID-19 patients are shocked when they find out that they will die. In 1918, people respected and valued doctors, but the life expectancy for men was 36.6 years, and 42.2 for women. People didn’t feel as invulnerable -and didn’t assume that the hospital would save them- because they were more familiar with death. In 1917 -the year before the pandemic- the second most common cause of death in the US was pneumonia and influenza.
Of course, in 1918 people relied heavily on newspapers and the government for information, whereas now people turn to social media. But I think that people were more familiar with infectious illness in 1918, and experienced the pandemic in a different way than with COVID-19. This difference perhaps helps to explain why in many states people seem to be much less afraid of COVID-19 than their great-grandparents were during the 1918 pandemic.
Shawn Smallman
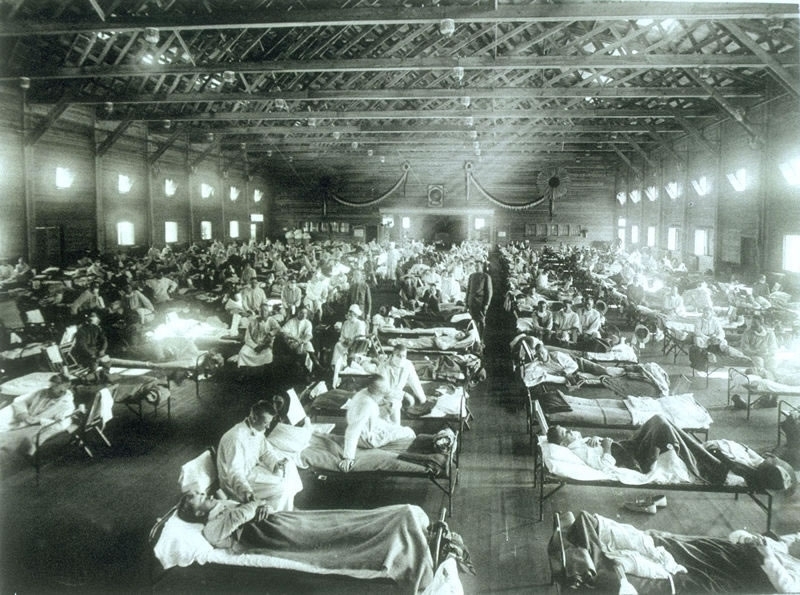
Historical photo of the 1918 Spanish influenza ward at Camp Funston, Kansas, showing the many patients ill with the flu- U.S. Army photographer
Recently I’ve been reading a book (published in 2004) by Betty O’Keefe and Ian McDonald titled, Dr Fred and the Spanish Lady. The work examines the experience of Dr. Fred Underhill, who was the senior public health officer in Vancouver during the 1918 pandemic. While there had been a host of influenza pandemics through history, the 1918 pandemic killed perhaps 100 million people globally.
What struck me while reading the work was the manifold similarities between our experience of COVID-19 and that of almost exactly a century before. During our current pandemic some countries, such as Australia, New Zealand and Taiwan, acted quickly to enact travel restrictions. But that was the exception rather than the norm. Similarly, in 1918 troop ships brought influenza to Canada, even though during the crossings the ships would have to repeatedly stop for the burial of sea for returning soldiers (O-Keefe and MacDonald, 30-31). In 1918, travel restrictions were not implemented because everyone in Canada wanted to bring the troops home. While understandable, this was also tragic. During COVID-19 there were no effective limits on returning citizens in the United States, likely because there just was not enough public support for this measure. Of course, there were limits on non-citizens’ travel. But since the SARS-Cov2 virus does not discriminate based on citizenship, those countries that did not limit their citizen’s movement, and quarantine them on arrival, have paid a heavy price. …
Historical photo of the 1918 Spanish influenza ward at Camp Funston, Kansas, showing the many patients ill with the flu- U.S. Army photographer
After the wonderful histories of Alfred Crosby and John Barry, readers might wonder if there is truly anything new left to write about the 1918 influenza pandemic, which killed between 50 and 100 million people world-wide, at a time when the world’s population was much smaller. Laura Spinney’s detailed, beautifully written and insightful work shows how much study can yet be done on this topic.
As Spinney describes in the opening to her book, in the 1990s much of the writing on this pandemic had been done on Europe and the United States. Of course there were exceptions. In Canada Eileen Pettigrew created a rich narrative of people’s experiences from survivors accounts, while Betty O’Keefe and Ian MacDonald told the story of how medical officer Fred Underhill fought the disease in Vancouver, Canada. There were similar accounts of popular experiences with the pandemic in other countries, such as Australia and New Zealand. But voices in Asia, Latin America and Africa were often not included. Since the 1990s there has been a plethora of work in many different nations, at the same that scientific advances have made it possible to have a much better understanding of the pandemic.
Spinney’s history takes full advantage of this study. She also has a gift for seizing upon the lives of individuals to tell a broader story, whether it was a young man in Rio de Janeiro, Brazil or a scientist in Republican China. She weaves together these narratives to create an overarching view that is truly global. After reading the work I find myself curious to learn more details on individuals, such as a woman affected by the pandemic in South Africa, who then created a religious (and perhaps millenarian) movement.
While such individual accounts are powerful, I particularly like chapter fifteen, in which she described how the same virus had dramatically distinct impacts in different places. Why would the same disease cause mortality rates in excess of 80 percent in some remote Alaskan and Labradoran villages, and far lower rates elsewhere? Of course, the flu was not unique in this respect. I wrote an entire book trying to understand the diversity of HIV epidemics in Latin America. What is perhaps most striking to me is that after a century of earnest study, many of these questions remain unanswered.
What is clear was that the pandemic utterly devastated some locations. In Western Samoa, twenty-two percent of the population died. In the Pacific, on the island of Vanuatu perhaps 20 languages died because of the heavy mortality that the virus brought. Given Brazil’s catastrophic response to the COVID-19 pandemic, and the disproportionate impact that the virus is having on Brazil’s Indigenous peoples, might something similar happen in the Amazon rain forest now? As Spinney states, there was a strange paradox to the virus. Cities often saw high mortality rates, but isolation caused terrible vulnerabilities in remote communities.
What was also striking to me was her discussion of the influenza’s aftermath. In part, this was reflected in such societal trends as a loss of faith in science. Will we be struck by a similar trend with COVID-19? But there was also a physical legacy of the virus, as many people suffered either psychological trauma over the loss of loved ones, or debilitating physical effects that lingered long after the virus was gone. Of these, perhaps the most famous was encephalitis lethargica. While it cannot be proven that the 1918 influenza pandemic caused this disorder -again so much remains unknown about this tragedy- the onset of the one was accompanied by the emergence of the other, as some people remained paralyzed -but apparently aware- for decades. Will COVID-19 have similar health effects that linger for more than a generation? The thought is chilling, given that one recent pre-publication from Korea just reported that up to 90 percent of COVID-19 survivors still report symptoms months later.
Still, what most struck me is that we are now having the same debates now that we had over a century ago: “One 2007 study showed that public health measures such as banning mass gatherings and imposing the wearing of masks collectively cut the death toll in some American cities by up to 50 percent (the US was much better at imposing such measures than Europe).” While now it is the US struggling to persuade its citizenry to wear masks, there is a haunting quality to the debates from this time. Some challenges that faced public health authorities then echo during the COVID-19 pandemic now, although (as far as I know) the death threats and public vilification of public health leaders was uncommon in America a century ago. So perhaps things have gotten worse. Spinney’s last two chapters are remarkably prescient for a book that was published in 2018.
I’ve spend much of the last twenty years working on public policy and infectious disease, first with my book on HIV/AIDS, and more recently with Zika and avian influenza. Some factors are constant, such as the fact that conspiracy theories emerge with every pandemic. One of the most common human urges when faced with an outbreak is to find someone to blame. But what depresses me is that I don’t think the historical studies or public policy achievements make much difference in the long run. In 2018 I published an article on wet markets in Hong Kong, which recommended that the special administrative region consider closing them. Of course, COVID-19 did not emerge in Hong Kong, but likely from a wet market in eastern China. One of the reasons that I hate conspiracy theories is that the distract from the real actions that could make people safer. They also make pandemics and outbreaks seem mysterious and unpredictable.
In fact, people have been studying coronaviruses in China since SARS emerged in 2003 precisely because such an event might take place. This was entirely predictable. As I said in an earlier blog post, how much human suffering might have been avoided if China’s wild game markets -which particularly cater to an older and wealthier clientele- had been closed. Yet even the Chinese government -with all its power and influence- either would not or could not do this. And now social media accounts spread tales that this outbreak is caused by 5G, and people in Britain burn cell towers. Two million people have died globally and winter is drawing closer in the northern hemisphere. We all know what happened in November 1918. Now we must now hope that a different virus will have a dissimilar impact.
Yet behind the scenes scientists have laid the groundwork that will allow for vaccines to be more quickly developed, because much basic science work has been completed. For all the frustration with sciences’ failures and limitations, the hope that we have now doesn’t come from conspiracy narratives -which don’t lead to any constructive steps- but from the often ignored work by nearly anonymous scientists in global laboratories. This work lacks the drama of the conspiracy theories, but the time-consuming and methodical study has laid the groundwork for the greatest vaccine push in human history. Conspiracy theories are easy to create. Real public policy or scientific advances are far more difficult, time-consuming and (often) difficult to understand. Spinney’s work is built upon a detailed examination of both the historical and scientific literature that has been built up over the last century, particularly the last twenty years.
It has long gone out of fashion in academia to look for lessons or a moral in history. But if this line of thinking is taken too far, it might lead people to question the value of history entirely. If historical study cannot give us lessons for the present period, isn’t it little more than a hobby for the affluent few? Laura Spinney’s brilliant book shows how a careful understanding of history can provide us the context to better understand current challenges. Sadly, in this current moment, it’s probably difficult to interest people in reading a work about a past outbreak. Spinney’s magisterial, carefully researched and beautifully written book deserves a broad audience. Highly recommended.
References
Spinney, Laura. Pale Rider : The Spanish Flu of 1918 and How It Changed the World. First US Trade Paperback ed. New York: PublicAffairs, 2018.
See also the following works for more reading on this topic.
Barry, John M. The Great Influenza : The Epic Story of the Deadliest Plague in History. New York: Viking, 2004.
Crosby, Alfred W. America’s Forgotten Pandemic. West Nyack: Cambridge University Press, 2003.
Canadian popular histories:
O’Keefe, Betty, and Ian Macdonald. Dr. Fred and the Spanish lady: Fighting the killer flu. Heritage House Publishing Co, 2004. (Full disclosure: this press also published my history of an evil spirit in Algonquian belief. Please note that I have no control over the price of physical copies of this book on Amazon, which sometimes surges to hundreds of dollars for mysterious reasons. So if you click on this link for my book, please don’t send me unhappy emails to complain about the book’s price).
Pettigrew, Eileen The silent enemy: Canada and the deadly flu of 1918. Saskatoon: Western Producer Prairie Books, 1983.
Map of Hong Kong by Shawn Smallman, Apple pencil in Procreate
This week I had an article published: “Wet Markets and Avian Influenza: Public Policy Decisions in Hong Kong.” Because the Journal of International and Global Studies is open source, you can read the article by clicking on the link above if you are interested. You can also read the abstract here:
After the emergence of H5N1 avian influenza in 1997 Hong Kong implemented a sophisticated system to regulate live poultry markets. While this system is well designed and thorough, it also has limitations. The rise of H7N9 avian influenza (which is typically acquired through contact with poultry, including in live markets) makes this an appropriate time to revisit the ethical and practical issues related to this trade. Based on data from field observations of live markets in Hong Kong, and interviews with experts in the field, this paper recommends that the government of Hong Kong create a committee to examine the pros and cons of ending live poultry markets in this Special Administrative Region.
The 1918 influenza pandemic was the disease outbreak that took the greatest toll in the twentieth century. Globally, perhaps between fifty and a hundred million people died. There are a wealth of wonderful books on the topic. I particularly recommend both Alfred Crosby, America’s Forgotten Pandemic and John Barry, The Great Influenza. Eileen Pettigrew’s Silent Enemy is an excellent popular account of Canada’s experience of the pandemic.
Years ago I was visiting a graveyard in Portland, Oregon. There were three graves next to each other, a man, a woman, and a child, who had all died within a few days of each other in November, 1918, almost certainly from the flu. It’s hard to imagine now what that lived experience must have been like. So many families have stories of ancestors who fought in World War One and survived, only to die on their way home.
My own grandfather was traveling in the Peace River country of northern Alberta at the time. He had decided that he was bored on the farm in southern Ontario. He and a friend had set out on an adventure to travel to the Yukon. Then his friend came down with the flu that fall in 1918. Although they never did make it to the Yukon, my grandfather helped to get his friend Frank home, where -as far as I know- he had a long and happy life. Of course, this was only one insignificant moment in the global disaster that impacted families from India to Australia, and took tens of millions of lives.
There is a fascinating new podcast series on this outbreak, which is well-researched and thoughtfully presented: Going Viral: the Mother of All Pandemics. The presenters have deep historical knowledge, and have invested an immense amount of time in preparing this engaging work. I enjoyed their trip to the former battlefields of France to try to track down the pandemic’s origin with Dr. John Oxford. One would think that there wasn’t much new left to say on this topic. Yet in their search for the true origins of the pandemic they look at provocative thinking and current debates, such as Mark Osborne Humphries’ idea that perhaps the pandemic actually began in China. They are also engaging speakers; one can imagine listening to them as a student, and being captured by their lecture style. You can find the podcast on iTunes and similar venues. Given the proliferation of H7N9, the diversification of influenza clades, and the fact that we still don’t have a universal influenza vaccine, this history remains sadly relevant. Highly Recommended. If you are interested to learn about more recent debates, you can also read my own work on influenza and pre-pandemic vaccines as well as conspiracy theories. Both of these articles are publicly available for free. You can also find more freely available articles on influenza here.
The 2009 pandemic of H1N1 influenza led people around the globe to create narratives about the epidemic defined by the question of trust; these narratives ranged from true conspiracy theories to simply accounts in which mistrust and betrayal formed a motif. In particular, most of these narratives reflected a fear of capitalism and globalization, although in specific regions, other issues—such as religion—played a more central role. These stories were not unique to the H1N1 pandemic but rather have appeared with every contemporary outbreak of infectious disease. This paper will examine conspiracy theories and moral panics related to the H1N1 pandemic in different world regions to explore how the disease became associated with economic and social systems in these accounts.
While many factors are driving the current protests in Iran, Michael Coston has pointed out that a significant outbreak of avian influenza in that country has driven up the cost of poultry and eggs, which has likely contributed to peoples’ food insecurity. His blog post is an interesting attempt to tie influenza to economic factors, which in turn may be connected to politics.
The Journal of International and Global Studies is an open access journal, which has just published my article: Whom do you trust: Doubt and Conspiracy theories in the 2009 Influenza Pandemic. The article examines how people in widely separated world regions responded to the pandemic with motifs based around trust and betrayal. While the article focuses on influenza, it also discusses other diseases such as polio and Ebola. Currently the Ebola in West Africa has been waning, and Liberia has finally been declared to be free of the disease. Even now, however, public health workers have to struggle against a powerful narrative of denial, which depicts Ebola as a tool created by the West to sell expensive medications. As I discuss in the article, such narratives have deep roots.
Shawn Smallman
Randall Munroe, XKCD Creative Commons Attribution and non-commercial use 2.5 license
As Americans and Canadians follow the threats posed by emerging infectious diseases they are accustomed to hearing news from distant countries such as Saudi Arabia or Liberia. While the threat posed by highly pathogenic avian influenza (HPAI) may move its focus from Indonesia to Egypt, events seem far from our borders. Yet the U.S. is now in the midst of a grave outbreak of HPAI, which is devastating flocks in the Midwest. While this is primarily an avian disease, there is always the risk that it may jump to humans. Even if it remains confined to poultry, the long-term economic effects are serious. The virus is unlikely to disappear or be eradicated at any time in the near future. As always, Maryn McKenna is one of the best observers of issues related to infectious disease. I highly recommend her recent article on this topic here. It’s important to note that there is no evidence that the virus is transmitting from birds to humans at the current time, and that the CDC is preparing a vaccine, just in case. As others have noted, the larger issue is the sheer number of HPAI strains circulating globally, which is very different from even a decade ago.
The French website Sentiweb tracks disease prevalence in the country. This winter the map of influenza-like illness in France has been a sea of red, which documents a particularly bad year. The situation in Germany is no better. Influenza viruses mutate over time, which means that every year vaccine makers must guess which strain of the virus is most likely to cause illness in the coming season. Sadly, this year’s vaccine was poorly matched with the strain of H3N2 that has caused the most illness. According to a study in the U.S. it was only 23% effective, while one study in Canada found that people were actually more likely to become ill if they had been vaccinated. You can’t have a much worse vaccine that that. This situation has meant that more people in the United States went to the hospital with an influenza-like illness than in most years, particularly amongst the elderly. At least in the United States the influenza season is now waning. In my home state of Oregon, influenza cases peaked last month. This sadly does not seem to be the case in France as this map suggests. As in the United States, the majority of cases in France have been the H3N2 strain.
People tend not to treat influenza with sufficient respect. Years ago I had a phone call from someone who wanted to drive to Portland to meet me in my role as the Director of International Studies. The morning of the meeting I woke up and knew right away that I had the flu. It felt as though somebody had turned up the gravity in my room. I had a high fever and could barely stand. But not wanting to disappoint them, I dragged myself to the office. They didn’t show up, and after an hour I went home. I consoled myself that it was for the best, because they last thing that they needed was to catch my flu. …