For the last twenty years or more I have been doing work on public health. A key part of that work has been studying conspiracy theories during pandemics. I first started working on this topic when I was doing research on HIV/AIDS in Latin America. While I spent time in Brazil, Cuba and Mexico, I heard many conspiracy theories about HIV/AIDS: it was designed in a US military lab to control populations in developing countries or that pharmaceutical companies had found a cure that they kept secret to ensure their profits from HIV treatments. Upon returning home I heard a great deal of HIV denialism -the belief that AIDS was not caused by a virus- in my classes from my students. It’s hard to believe now, but twenty years ago there were many students who would argue passionately that HIV was caused by drugs or pesticides sold by Monsanto.
In the years that have followed I have written about the conspiracy theories that have surrounded everything from Zika to the 2009 influenza pandemic. What has always struck me about these conspiracy theories is how much recycling they entail. The same narratives are reused no matter the new health threat that emerges. Sometimes I think that I have worked on this topic for too long, and that I am at risk of repeating my own arguments. But these theories matter. Why would a pregnant women in a Zika affected area put on insect repellent if she doesn’t believe that the vector is a mosquito?
Ebola is a classic example of the damage these theories can cause. I have a new paper out that asks why there was such a difference in how social media companies responded to conspiracy theories about Ebola and COVID. It’s a brief essay but I hope that it will provoke some discussion.
Shawn Smallman, 2023
Smallman S. Conspiracy Theories and Ebola: Lessons Learned Important for Future Pandemics. Norton Healthcare Medical Journal. 2023; 1(1). doi:10.59541/001c.77445
Early in the pandemic I thought it likely that COVID-19 would have multiple waves, perhaps three like the 1918 influenza pandemic. So I never thought that the pandemic would end quickly. But over the last six or seven months I keep finding myself thinking that this time, finally, it must be ending. In June I had both of my COVID-19 vaccinations, cases in the US were plummeting, and I thought that by this winter it would have finally ended. Then Delta arrived, and filled the emergency rooms of the US south. This fall I was able to travel to Lisbon, where I am carrying out historical research on the 1918 influenza pandemic. When I arrived this October Portugal was the most vaccinated country in Europe, and was the subject of a front page article in the New York Times. And yet since I’ve arrived I’ve seen the case right rise dramatically. Not long ago I was looking at the New York Times country data page, and saw that cases in Portugal had increased 116% in two weeks. The country’s case rate may pass that of the US before long. Keep in mind that not only does Portugal have a high vaccination rate, but also people are very good about wearing masks here. It’s common to even see people wearing them in the street, at least if the street is crowded.
While Portugal is facing serious challenges, the situation is far better here than it is in other places, such as Austria. The COVID-19 incidence there is growing at a stunning rate. The government is implementing firm measures, but is facing mass protests. Other countries, such as the Netherlands, are in the same situation, as we have seen from the protests in Rotterdam. Still, the situation is much worse in Eastern Europe, where in some countries such as Bulgaria only a quarter of adults are vaccinated.
It’s in this context that we are receiving news about a new -as yet unnamed- variant in South Africa. There is a lot that we don’t know about this variant yet. The German news channel recently interviewed one expert who suggested that it might be 500 percent more infectious than Delta, although he stressed that we just don’t know yet. Even such qualified statements are dangerous. We will have more data soon. Still, there is a lot of speculation that this variant might partially evade vaccines, because there are so many mutations, including a number involving the virus’s spike protein.
Nations are rushing to block flights from South Africa. Britain was very slow to respond to the Delta variant, and allowed travel to continue for weeks after it was clear that Delta might lead to a new wave. But after the news of this new variant emerged Britain blocked air travel from Southern Africa. Many other nations are also imposing travel restrictions. Of course, this variant has already been found in Israel. And in Hong Kong -where it was brought by a traveler from South Africa- it managed to spread to one other person in a quarantine hotel. Blocking travel from South Africa will help to buy some time, which might be put to use gathering data on the virus. It might also give people the time to be fully vaccinated and get their boosters, if they are in countries in which vaccines are readily available. But in the end, it won’t be enough. Without a complete border and air travel shut down, a highly infectious virus will certainly spread globally.
Given that Delta is already so severe in Europe, the timing for the emergence of this variant could not be worse for this region as it heads into winter. People are exhausted from the pandemic. But it’s not over. Please, if you are not vaccinated, hurry to be vaccinated now, so that your body has time to build immunity. While all medical treatments have risks, the risks of COVID-19 are much greater, billions of people have had the vaccines, and a new variant is coming. And if you are eligible for a booster, now would also be a good moment for that too. Two months ago there was a significant debate around whether boosters were necessary. Given what’s happening now in places like Portugal, there’s no doubt that only focusing on the severity of cases, and not on transmission, is a poor public health approach.
Let’s hope that this proves to be a false alarm, and that the new variant doesn’t greatly increase severity, transmission, or vaccine evasion. We all deserve some luck.
On October 6, 2021 the World Health Organization made a historic announcement. They had approved the world’s first malaria vaccine, which had been in development for more than thirty years. Of course, this amount of time is trivial compared to the history of malaria itself. The disease is one of humanity’s oldest scourges. There are tombs along the Nile that hold mummies who died of malaria. As Rome collapsed in the late fourth and fifth century malaria ravaged Italy, and depopulated entire regions. When a Spanish conquistador descended the Amazon river from Peru to the Atlantic, the friar Carvajal reported that the river bank was so densely settled that each town lay only a crossbow shot from the next one. A hundred years later these communities had vanished. And even today in Africa and southeast Asia every year hundreds of thousands of children either die or are left with life long disabilities (such as epilepsy) from the disease. In many regions, it’s almost impossible to avoid, although the WHO has put great effort into promoting sleeping nets and insecticides.
I recently did a podcast interview with Dr. Marylynn Steckley, who talked about her experience researching in Haiti, while both she and her family suffered from frequent illness. Malaria makes some parts of the world difficult to live and work in for everyone, including outsiders. Although I have not had malaria, I have known many people who have, and for whom it had an enduring impact on their health. Indeed, for many of my Africanist colleagues it was almost assumed that they would acquire the disease, and perhaps live with it’s long term effects. Some of my African colleagues -such as one archaeologist- have many stories about their bouts with the disease.
It’s ironic that during this terrible COVID-19 pandemic we finally have some positive news. This is not only the first vaccine against malaria, but -as many observers note- the first against any parasitic disease. As such, it’s a proof of principle. Some people have wondered if it might prove to be impossible to develop vaccines against these class of diseases, since parasites have evolved to overcome the human immune system for long periods of time. Now we have seen that it can be done.
The vaccine is known as RTS,S/AS01, and it has its limitations. It’s only effective around 40% of the time. It also requires four doses. Even so, given that more 200 million people a year are infected with malaria, this can prevent an immense amount of suffering. More vaccines are in the development process.
There is something remarkable about this new vaccine. It relies on an ingredient from an evergreen tree (the quillay tree) that grows in only one place in the world, Chile on the Pacific coast of South America. This rare ingredient is an adjuvant, which is an ingredient in a vaccine that helps to create an immune response in the human body. The first useful medication for malaria was quinine, which comes from a tree grown in the Amazonian region. Now, once again, Indigenous knowledge and a South American plant, is proving vital in the struggle against malaria. It also places intense pressure upon the stocks of the quillay trees, especially as this ingredient is also being used to develop at least one COVID-19 vaccine and a shingles vaccination. There is currently a technological race on to understand how to extract this ingredient from seeds and immature Quillay trees, because currently the supply replies upon mature trees of at least thirty years of age.
Humanity still has a long way to go in this fight against a killer that even affected pharaohs. But -with help from an usual Latin American tree- the world has its first vaccine, and that is an immense step forward.
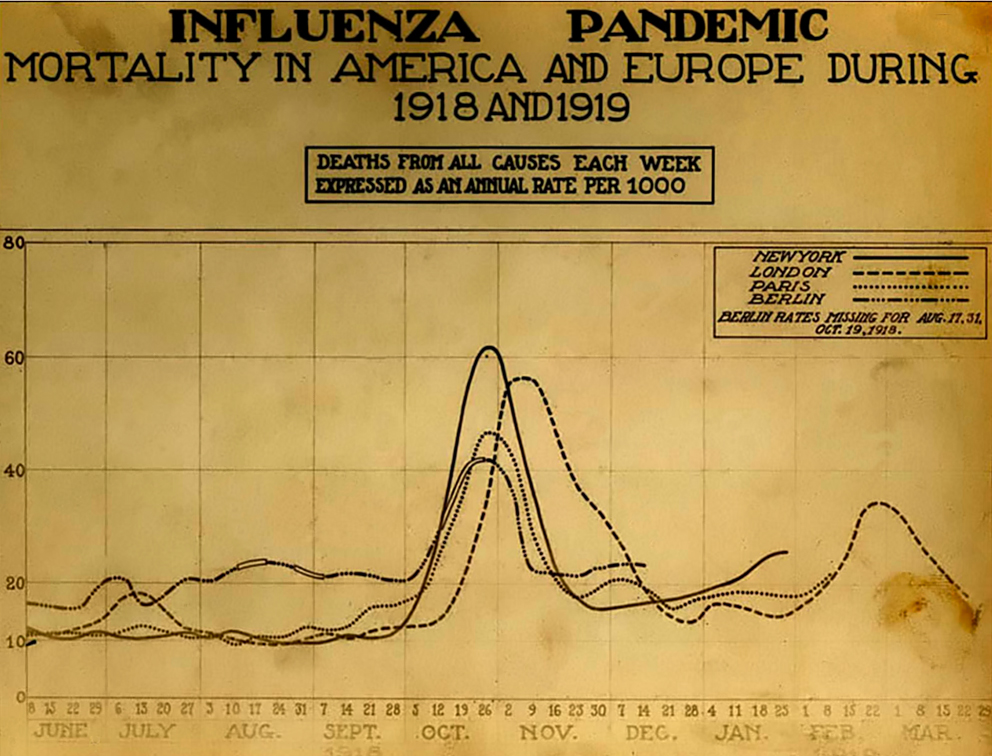
The Spanish Influenza. Chart showing mortality from the 1918 influenza pandemic in the US and Europe. Wikipedia commons.
According to the CDC, as of September 10, 2021, 652,480 Americans had died of COVID-19. This is nearly as many as the perhaps 675,000 Americans who died in the 1918 flu pandemic. But there seems to be much less fear of COVID-19 now than there was of the influenza pandemic then, at least in some parts of the United States. Why?
Of course, the first point to make is that there was certainly denial and minimizing in the United States in 1918, which people used to justify holding everything from war-bond rallies to weddings. Still, after the terrible month of November 1918 this declined. Is the difference between then and now in part that we live in social media bubbles? I think that there is some truth to this, but there are a few factors that explain the different attitude that many people had towards influenza then.
In 1918, there was a “W” shaped mortality curve, as most people who died were infants, young adults and the elderly. Before the arrival of the delta variant, there was a perception that those people most at risk of COVID-19 were over 65, and perhaps their deaths were less shocking. In contrast, younger people felt relatively safe. In 1918 it was people in the prime of their life who were dying, as well as their children. This made people feel more vulnerable.
Today, people typically die in the hospital. In 1918, if you lived in a rural area -as did most of the population- a trip to the hospital would take time and might not be easy. More people were cared for –and died– at home. I think that this meant that people saw the results of outbreak much more directly. Today, the ill vanish into hospitals. Their suffering leaves nurses and doctors traumatized, but isn’t visible in the same way that the 1918 pandemic was, when family members and neighbors would see the bodies taken out the front door.
There were three distinct waves to the 1918 influenza pandemic. But the fall 1918 wave had a much higher peak in the death rate. Of course, the spring 1918 influenza outbreak was terrible in some places such as the military camps in Kansas. But by November 1918 the number of deaths was so crushing that denial was no longer an option in many communities. People were too busy taking care of their neighbors; everyone could watch the gravediggers. COVID-19 has been more spread out, which has changed how people have talked about it.
The US population was much smaller in 1918 than now, at just over 103 million people, versus 328.2 million. So although the total numbers of deaths are similar, the death rate was roughly three times higher a century ago. People saw much more death during the 1918 pandemic.
I also wonder if people didn’t have a different attitude towards medicine. The 1918 pandemic took place before most childhood vaccines, antibiotics, and modern therapies. People had more limited expectations for what a doctor might do. Now, it might be that many people expect that if they go to the hospital they will be saved, because they have often seen sick family members or friends healed in a hospital. I can’t prove this, but I suspect some COVID-19 patients are shocked when they find out that they will die. In 1918, people respected and valued doctors, but the life expectancy for men was 36.6 years, and 42.2 for women. People didn’t feel as invulnerable -and didn’t assume that the hospital would save them- because they were more familiar with death. In 1917 -the year before the pandemic- the second most common cause of death in the US was pneumonia and influenza.
Of course, in 1918 people relied heavily on newspapers and the government for information, whereas now people turn to social media. But I think that people were more familiar with infectious illness in 1918, and experienced the pandemic in a different way than with COVID-19. This difference perhaps helps to explain why in many states people seem to be much less afraid of COVID-19 than their great-grandparents were during the 1918 pandemic.
Shawn Smallman
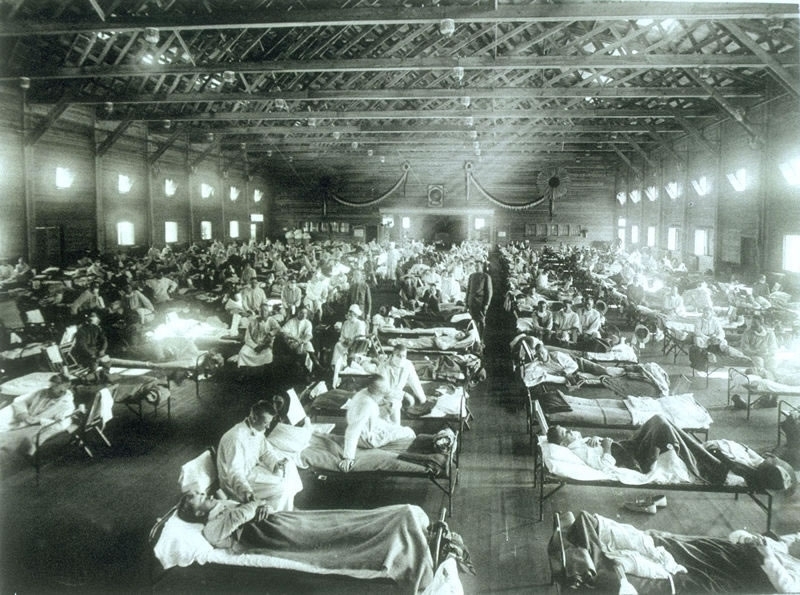
Historical photo of the 1918 Spanish influenza ward at Camp Funston, Kansas, showing the many patients ill with the flu- U.S. Army photographer
In November and December 2019 a novel corona virus began circulating in China. The world -and China’s citizens- first learned of this thanks to a group of Chinese whistle blowers , including Opthamologist Dr Li Wenliang, who would ultimately die of the virus. These whistle blowers were denounced by their administrators and some of them -such as Dr. Wenliang- received a police warning. After he died from COVID-19 on February 7, 2020 there was a wave of popular outrage, and sympathy for his pregnant widow, which caused authorities to censor Chinese social media platforms. So the Chinese state sought to conceal the COVID-19 outbreak in its early stages, much as it once did with SARS. But where did the virus come from? And what do we know about its origins?
Wet markets have often been associated with the start of earlier outbreaks of infectious diseases, such as avian influenza and SARS. This makes sense because these environments bring together a diversity of wild animals that may carry unknown pathogens. Packed into cages in poorly ventilated areas, viruses can passage across the species barrier in a way that would be difficult to achieve in the wild. When the outbreak first appeared in China, many people first looked at cases that appeared to be associated with a local wet market. But as earlier cases became known, the tie to the wet market lacked strong support in the data, although a recent study perhaps strengthens this case.
Attention turned to the Wuhan Institute of Virology (WIV), which reportedly had collected novel bat viruses, including some from a cave in Yunnan. Lab leaks have caused pandemics before. For example, in 1977 an influenza pandemic swept the world. Because the virus was nearly identical to historical samples from an earlier outbreak, there have been suspicions that it began as a result of a lab leak in the Soviet Union. Gain of function experiments -in which scientists deliberately increase either the transmissibility or infectiousness of an infectious agent have been controversial for many years for this reason. Accidents have happened.
Nearly a decade ago I was attending an influenza conference in Oxford, and happened to have breakfast with three well-known figures in the field of influenza virology. One of the people at the table was an outspoken advocate for gain of function research. This person’s work had attracted international controversy on this issue. He/she was an outspoken, confident person, who was more than willing to talk about the gain of function debate, and appeared to enjoy both the attention and the controversy. I thought that this person was eloquent, informed and generous in sharing their thoughts with a complete nobody like me. I was enjoying the conversation immensely. But as the discussion went on, another person at the table -a legend in influenza virology- became increasingly glum looking as he or she picked at their eggs. I felt increasingly awkward, and noticed that my charming colleague didn’t seem to be noticing their colleagues’ withdrawal from the conversation.
Finally, the gain of function researcher turned to another person -a German colleague- and said words to the effect: “You understand how these constraints are maddening.” And this German researcher said (as best as I can recall): “Yes, but I don’t do anything nearly as dangerous as you do.” One thing that I loved when I used to lecture in Germany (actually, I loved everything about Germany) was how frank my students were in giving feedback, and this response was true to form. What I took from the debate was the extent to which gain of function research worried even those people with the best practical knowledge of laboratory work with influenza viruses. As time has passed, there has been increasingly skepticism that gain of function research will produce knowledge at all worthy of the risks. But did the Wuhan Institute of Virology in fact have novel corona virus sequences, and -if so- what kind of research was being done with these strains? …
Every pandemic leaves in its wake people who survived, but were changed by their infection. The most famous example of this is likely encephalitis lethargica, which famously reduced some people to living in a near coma after they survived the 1918 influenza pandemic. For decades some people have been arguing that Chronic Fatigue Syndrome (and perhaps chronic Lyme disease) are also caused by viruses and bacteria, which cause immense but hidden damage in the body. These sequelae endure after the initial infection subsides. Over the last several months many people who were infected by COVID-19 have developed long COVID, a syndrome that remains a medical mystery. One of my favorite new podcasts is Unexplainable, which looks at scientific mysteries. Their recent episode, “The Viral Ghosts of Long COVID” paints an unsettling picture of this disorder. The podcast begins with someone describing the long term effects of their Ebola infection, which closely resemble the symptoms reported by COVID survivors. Many people now wonder whether more research on Chronic Fatigue Syndrome earlier might not have made us better prepared to face this new challenge now.
Recently I’ve been reading a book (published in 2004) by Betty O’Keefe and Ian McDonald titled, Dr Fred and the Spanish Lady. The work examines the experience of Dr. Fred Underhill, who was the senior public health officer in Vancouver during the 1918 pandemic. While there had been a host of influenza pandemics through history, the 1918 pandemic killed perhaps 100 million people globally.
What struck me while reading the work was the manifold similarities between our experience of COVID-19 and that of almost exactly a century before. During our current pandemic some countries, such as Australia, New Zealand and Taiwan, acted quickly to enact travel restrictions. But that was the exception rather than the norm. Similarly, in 1918 troop ships brought influenza to Canada, even though during the crossings the ships would have to repeatedly stop for the burial of sea for returning soldiers (O-Keefe and MacDonald, 30-31). In 1918, travel restrictions were not implemented because everyone in Canada wanted to bring the troops home. While understandable, this was also tragic. During COVID-19 there were no effective limits on returning citizens in the United States, likely because there just was not enough public support for this measure. Of course, there were limits on non-citizens’ travel. But since the SARS-Cov2 virus does not discriminate based on citizenship, those countries that did not limit their citizen’s movement, and quarantine them on arrival, have paid a heavy price. …
Mercator Map of the Congo, 1595, from the Northwestern University Library Maps of Africa collection, accessed through Wikipedia.
I wrote a book, the AIDS Pandemic in Latin America, and have studied public policy and infectious disease for nearly twenty years. Here is a lecture that I wrote (around 2010?) for an “Introduction to International Studies” class. It would need to be updated now; it may also some references to my own experiences, which would need to be removed. But my hope is that it might prove a useful starting place for someone who wants to do a lecture on this topic in a similar class.
Next Tuesday my department will be having a presentation on Zoom about COVID-19 in Latin America. During this discussion I’ll be talking about Bolsonaro’s leadership in Brazil, and the current pandemic trends in that country. Dr. Rodriguez will be talking about Argentina’s response, while Dr. Young will be discussing the experience of both Cuba and Mexico. Since I know little about the COVID-19 situation outside of Brazil in Latin America, I am particularly interested to hear what my co-presenters will say. The talk will be 2pm West Coast (US) time. Please RSVP if you are interested in participating.
Photo by Isabella Mori, who provides this context: In traditional Taiwanese night markets, since people / food stands are in close contacts, most people / vendors wear masks now, in order to protect themselves and others.