All around the developed world nations and local governments are trying to persuade people to go have a COVID-19 vaccination. Where I live, I am flooded with ads, which are mostly politicians and public health authorities. These ads mostly have a talking head format, so they don’t have a lot of visual interest. And no catchy songs. Then there is Singapore’s approach.
Singapore’s most recent ad highlights a comic duo, a musical number, uni-color background shots, Singlish and dance. I’m not sure where I first read about this two minute ad, but it shows another approach to public health communication. Here in the United States, I hope that we’ll see ads with football quarterbacks, basketball players, religious leaders, movie stars, musicians and others. People need to see spokespeople supporting the vaccine who aren’t epidemiologists. And maybe somebody else could do a musical about vaccinating. “Steady pom pi pi” everyone.
The early story of Britain’s reaction to COVID-19 was an unmitigated disaster, driven in part by uniformed cabinet discussions of herd immunity. Even Prime Minister Boris Johnston himself was infected with COVID-19. As if this story was not difficult enough, a new variant of COVID-19 appeared in Essex towards the end of 2020. We now know that not only is this variant more communicable, but also may be more deadly. In late December this virus came to dominate all the COVID-19 clades in Britain, and caused a remarkable surge in infections.
In spite of this difficult history, Britain has pulled of two remarkable achievements. First, it has conducted outstanding genomic surveillance. While Denmark was also doing so, it was the British tracking which revealed the extent of the threat these new variants posed. Now other nations, such as the United States, are playing catch-up, as they try to create an effective system for genomic surveillance. Even more remarkable, Britain has joined a short list of nations (along with Israel and the United Arab Emirates) leading the global race to vaccinate their populations. How was this success achieved?
Paul Waldie has a remarkable article in Canada’s Globe and Mail, titled “How Britain became a world leader in COVID-19 vaccine distribution – despite other pandemic problems.” In Waldie’s narrative one remarkable woman, Kate Bingham, and the task force that she led, managed to identify the likely winners in the vaccine race, negotiate contracts, and bring vaccine production home to Britain. What is most impressive is how proactive the task force was. Britain has had many missteps and still faces many challenges. Yet when the history of this pandemic is written, I think that -based on Waldie’s description- this task forces’ actions will be held up as a case-study of effective leadership during a crisis.
Recently I’ve been reading a book (published in 2004) by Betty O’Keefe and Ian McDonald titled, Dr Fred and the Spanish Lady. The work examines the experience of Dr. Fred Underhill, who was the senior public health officer in Vancouver during the 1918 pandemic. While there had been a host of influenza pandemics through history, the 1918 pandemic killed perhaps 100 million people globally.
What struck me while reading the work was the manifold similarities between our experience of COVID-19 and that of almost exactly a century before. During our current pandemic some countries, such as Australia, New Zealand and Taiwan, acted quickly to enact travel restrictions. But that was the exception rather than the norm. Similarly, in 1918 troop ships brought influenza to Canada, even though during the crossings the ships would have to repeatedly stop for the burial of sea for returning soldiers (O-Keefe and MacDonald, 30-31). In 1918, travel restrictions were not implemented because everyone in Canada wanted to bring the troops home. While understandable, this was also tragic. During COVID-19 there were no effective limits on returning citizens in the United States, likely because there just was not enough public support for this measure. Of course, there were limits on non-citizens’ travel. But since the SARS-Cov2 virus does not discriminate based on citizenship, those countries that did not limit their citizen’s movement, and quarantine them on arrival, have paid a heavy price. …
Throughout the last several months, the US Center for Disease Control has messaged that in order to catch COVID-19 you had to be within six feet of an infected person for fifteen minutes. This was reassuring information. But sadly the US was also perhaps in a difficult place to answer detailed questions about COVID cases, because the contact tracing system has been overwhelmed. The US has also lacked a national COVID tracking app, as many other nations (Australia) have had. Realistically, this would have been a political impossibility to implement in the US, given that even masks have been highly politicized here. So, how realistic was the CDC’s guidance?
In Korea, contact tracing has been highly effective. It turns out that the combination of a digital tracking app with highly skilled contact tracers has been more successful than either purely digital or human tracing would be. And what Korea has learned -in a remarkable piece of scientific work- is that in one case a high school senior was infected after five minutes of exposure and from twenty feet away. The infection took place in a restaurant (which had video recording) and it turns out that an air conditioning unit was wafting air from an infected person towards the student. The quality of the data that the contact tracers obtained -and the history of how they learned it- is remarkable, and well worth reading.
There is nothing magic that happens at the six feet mark from another person. And being exposed to an infected person indoors can be risky even when the CDC’s old guidelines might make us feel safe. In this case, Korea has given us not only important information, but also let us see the quality of information contact tracing can provide. The key message is that neither six feet of distance, or avoiding more than fifteen minutes of exposure to another person, may be enough to keep you safe from infection, particularly indoors. So indoor dining is probably always unsafe.
Bust and Plaque at the Fighting SARS memorial, Hong Kong
A recent study published in the American Journal of Microbiology journal, MBIO, suggests that MMR 2 vaccine helps to prevent COVID-19 symptoms. It’s a study based on a small population (80), but the MMR blood titers show a very strong association with the severity of COVID-19 illness. People with high titers were all asymptomatic. Everyone who became severely ill had titers under 32. This wasn’t the first article exploring this idea of an association between MMR vaccination and COVID-19 resistance. But it’s an intriguing one that deserves more attention and research.
As a press release from the American Journal of Microbiology states, this could also explain why children don’t seem to get seriously ill. The MMR blood titers fall as you age. And the elderly may never have had this vaccine, in part because they’ve had measles or mumps. One significant point to the study was that having had the mumps doesn’t protect you. People need to have the vaccine itself. This contradicts the argument of vaccine critics who say that it’s better to have natural immunity. But in this case, the vaccine seems to give better immunity. As someone who had mumps as a child (and then gave it to my sister) I’m in favor of a vaccine-based approach to public health, rather than natural or herd-immunity.
I want to emphasize again that this study was based on the MMR blood titer results of only eighty people who had COVID-19. So this is a preliminary study. But the risks of the MMR are very low; at least hundreds of millions of people have had it since it was first introduced in 1971. Please note that this study only examined the MMR 2, not the quad vax, which also includes varicella.
Even though new COVID vaccines are coming soon, it will take months to roll the out at scale. It would be wonderful if we could use an existing vaccine with a long track record for safety to help us to buy time.
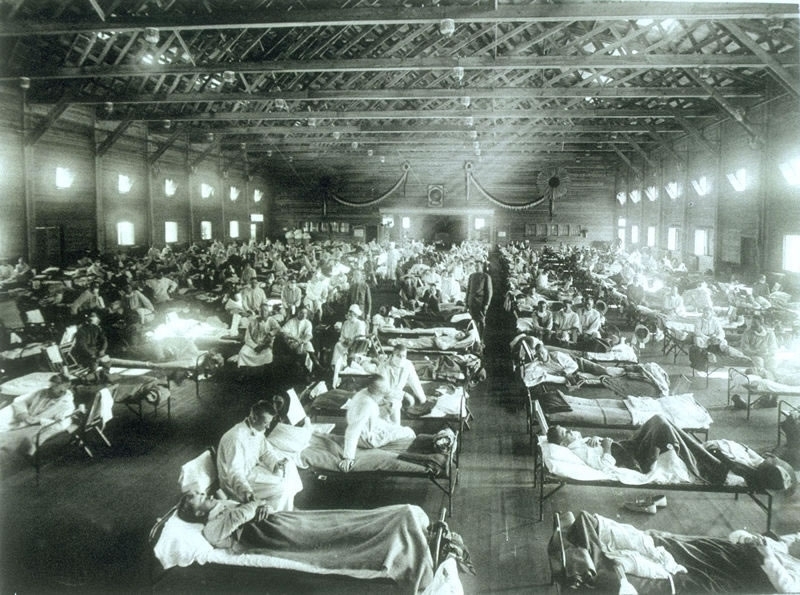
Historical photo of the 1918 Spanish influenza ward at Camp Funston, Kansas, showing the many patients ill with the flu- U.S. Army photographer
After the wonderful histories of Alfred Crosby and John Barry, readers might wonder if there is truly anything new left to write about the 1918 influenza pandemic, which killed between 50 and 100 million people world-wide, at a time when the world’s population was much smaller. Laura Spinney’s detailed, beautifully written and insightful work shows how much study can yet be done on this topic.
As Spinney describes in the opening to her book, in the 1990s much of the writing on this pandemic had been done on Europe and the United States. Of course there were exceptions. In Canada Eileen Pettigrew created a rich narrative of people’s experiences from survivors accounts, while Betty O’Keefe and Ian MacDonald told the story of how medical officer Fred Underhill fought the disease in Vancouver, Canada. There were similar accounts of popular experiences with the pandemic in other countries, such as Australia and New Zealand. But voices in Asia, Latin America and Africa were often not included. Since the 1990s there has been a plethora of work in many different nations, at the same that scientific advances have made it possible to have a much better understanding of the pandemic.
Spinney’s history takes full advantage of this study. She also has a gift for seizing upon the lives of individuals to tell a broader story, whether it was a young man in Rio de Janeiro, Brazil or a scientist in Republican China. She weaves together these narratives to create an overarching view that is truly global. After reading the work I find myself curious to learn more details on individuals, such as a woman affected by the pandemic in South Africa, who then created a religious (and perhaps millenarian) movement.
While such individual accounts are powerful, I particularly like chapter fifteen, in which she described how the same virus had dramatically distinct impacts in different places. Why would the same disease cause mortality rates in excess of 80 percent in some remote Alaskan and Labradoran villages, and far lower rates elsewhere? Of course, the flu was not unique in this respect. I wrote an entire book trying to understand the diversity of HIV epidemics in Latin America. What is perhaps most striking to me is that after a century of earnest study, many of these questions remain unanswered.
What is clear was that the pandemic utterly devastated some locations. In Western Samoa, twenty-two percent of the population died. In the Pacific, on the island of Vanuatu perhaps 20 languages died because of the heavy mortality that the virus brought. Given Brazil’s catastrophic response to the COVID-19 pandemic, and the disproportionate impact that the virus is having on Brazil’s Indigenous peoples, might something similar happen in the Amazon rain forest now? As Spinney states, there was a strange paradox to the virus. Cities often saw high mortality rates, but isolation caused terrible vulnerabilities in remote communities.
What was also striking to me was her discussion of the influenza’s aftermath. In part, this was reflected in such societal trends as a loss of faith in science. Will we be struck by a similar trend with COVID-19? But there was also a physical legacy of the virus, as many people suffered either psychological trauma over the loss of loved ones, or debilitating physical effects that lingered long after the virus was gone. Of these, perhaps the most famous was encephalitis lethargica. While it cannot be proven that the 1918 influenza pandemic caused this disorder -again so much remains unknown about this tragedy- the onset of the one was accompanied by the emergence of the other, as some people remained paralyzed -but apparently aware- for decades. Will COVID-19 have similar health effects that linger for more than a generation? The thought is chilling, given that one recent pre-publication from Korea just reported that up to 90 percent of COVID-19 survivors still report symptoms months later.
Still, what most struck me is that we are now having the same debates now that we had over a century ago: “One 2007 study showed that public health measures such as banning mass gatherings and imposing the wearing of masks collectively cut the death toll in some American cities by up to 50 percent (the US was much better at imposing such measures than Europe).” While now it is the US struggling to persuade its citizenry to wear masks, there is a haunting quality to the debates from this time. Some challenges that faced public health authorities then echo during the COVID-19 pandemic now, although (as far as I know) the death threats and public vilification of public health leaders was uncommon in America a century ago. So perhaps things have gotten worse. Spinney’s last two chapters are remarkably prescient for a book that was published in 2018.
I’ve spend much of the last twenty years working on public policy and infectious disease, first with my book on HIV/AIDS, and more recently with Zika and avian influenza. Some factors are constant, such as the fact that conspiracy theories emerge with every pandemic. One of the most common human urges when faced with an outbreak is to find someone to blame. But what depresses me is that I don’t think the historical studies or public policy achievements make much difference in the long run. In 2018 I published an article on wet markets in Hong Kong, which recommended that the special administrative region consider closing them. Of course, COVID-19 did not emerge in Hong Kong, but likely from a wet market in eastern China. One of the reasons that I hate conspiracy theories is that the distract from the real actions that could make people safer. They also make pandemics and outbreaks seem mysterious and unpredictable.
In fact, people have been studying coronaviruses in China since SARS emerged in 2003 precisely because such an event might take place. This was entirely predictable. As I said in an earlier blog post, how much human suffering might have been avoided if China’s wild game markets -which particularly cater to an older and wealthier clientele- had been closed. Yet even the Chinese government -with all its power and influence- either would not or could not do this. And now social media accounts spread tales that this outbreak is caused by 5G, and people in Britain burn cell towers. Two million people have died globally and winter is drawing closer in the northern hemisphere. We all know what happened in November 1918. Now we must now hope that a different virus will have a dissimilar impact.
Yet behind the scenes scientists have laid the groundwork that will allow for vaccines to be more quickly developed, because much basic science work has been completed. For all the frustration with sciences’ failures and limitations, the hope that we have now doesn’t come from conspiracy narratives -which don’t lead to any constructive steps- but from the often ignored work by nearly anonymous scientists in global laboratories. This work lacks the drama of the conspiracy theories, but the time-consuming and methodical study has laid the groundwork for the greatest vaccine push in human history. Conspiracy theories are easy to create. Real public policy or scientific advances are far more difficult, time-consuming and (often) difficult to understand. Spinney’s work is built upon a detailed examination of both the historical and scientific literature that has been built up over the last century, particularly the last twenty years.
It has long gone out of fashion in academia to look for lessons or a moral in history. But if this line of thinking is taken too far, it might lead people to question the value of history entirely. If historical study cannot give us lessons for the present period, isn’t it little more than a hobby for the affluent few? Laura Spinney’s brilliant book shows how a careful understanding of history can provide us the context to better understand current challenges. Sadly, in this current moment, it’s probably difficult to interest people in reading a work about a past outbreak. Spinney’s magisterial, carefully researched and beautifully written book deserves a broad audience. Highly recommended.
References
Spinney, Laura. Pale Rider : The Spanish Flu of 1918 and How It Changed the World. First US Trade Paperback ed. New York: PublicAffairs, 2018.
See also the following works for more reading on this topic.
Barry, John M. The Great Influenza : The Epic Story of the Deadliest Plague in History. New York: Viking, 2004.
Crosby, Alfred W. America’s Forgotten Pandemic. West Nyack: Cambridge University Press, 2003.
Canadian popular histories:
O’Keefe, Betty, and Ian Macdonald. Dr. Fred and the Spanish lady: Fighting the killer flu. Heritage House Publishing Co, 2004. (Full disclosure: this press also published my history of an evil spirit in Algonquian belief. Please note that I have no control over the price of physical copies of this book on Amazon, which sometimes surges to hundreds of dollars for mysterious reasons. So if you click on this link for my book, please don’t send me unhappy emails to complain about the book’s price).
Pettigrew, Eileen The silent enemy: Canada and the deadly flu of 1918. Saskatoon: Western Producer Prairie Books, 1983.
Mercator Map of the Congo, 1595, from the Northwestern University Library Maps of Africa collection, accessed through Wikipedia.
I wrote a book, the AIDS Pandemic in Latin America, and have studied public policy and infectious disease for nearly twenty years. Here is a lecture that I wrote (around 2010?) for an “Introduction to International Studies” class. It would need to be updated now; it may also some references to my own experiences, which would need to be removed. But my hope is that it might prove a useful starting place for someone who wants to do a lecture on this topic in a similar class.
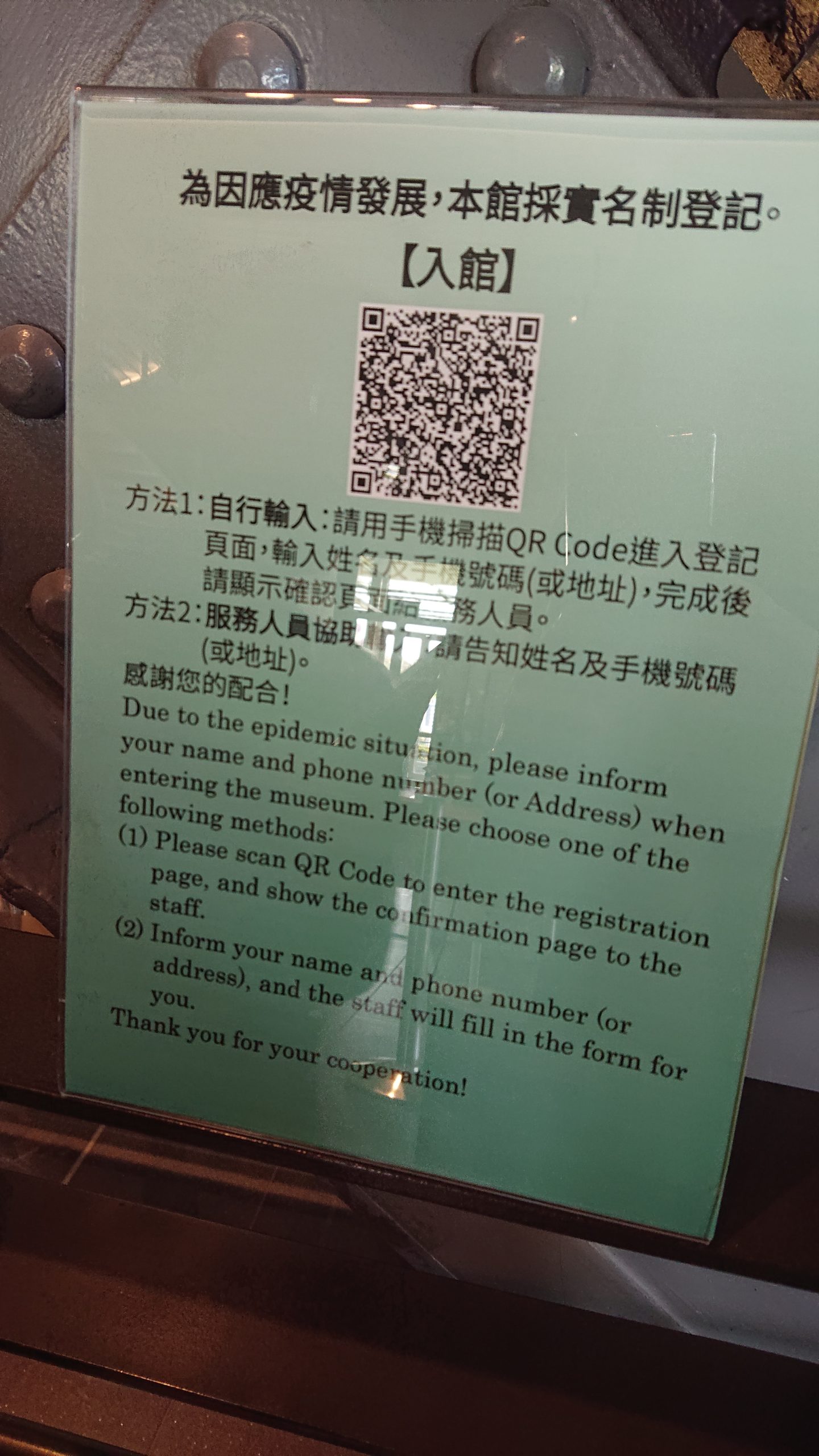
In Taiwan, before entering museums (and many other public institutions, offices, etc.), one needs to enter the Real-Name System (with one’s cellphone, by scanning the QR Code), on top of getting one’s temperature taken / sanitize hands with alcohol. By leaving one’s name and contact information, if a person got infected by COVID-19 and have been to the museum, the government will know who he / she have been in contact with. Photo by Isabella Mori.
One of the realizations that has come with COVID-19 is that the old binary between developed and developing countries is deeply flawed. Some nations that are less wealthy (Vietnam, Thailand) have succeeded very well in limiting the virus’s spread (at least in June 2020), while some wealthier countries (the United States and Great Britain saw their governments fail to control the outbreak, despite not only their relative wealth, but also sophisticated health care systems.
In the United States the CDC and FDA decided not to adopt a test for COVID-19 that was recommended by the World Health Organization (WHO). But their effort to create their own test was badly flawed. When that test proved not to work, it set the US testing back perhaps a month or more behind other nations at the most critical moment in the virus’s spread within the United States. In contrast, countries that adopted the WHO’s recommended test were able to test their populations at scale.
In Boston, there was a testing debacle after a number of people were infected at a Biogen conference. Even after people reported symptoms and repeatedly sought testing they were unable to be tested, because they did not meet the overly strict criteria that included travel to China, or contact with someone from China. The result was a disaster, which saw the outbreak flare so that Boston had one of the worst outbreaks in the world. Meanwhile, Vietnam carried out a very thorough testing program that has allowed to control the outbreak to this date.
One of the most interesting points for me has been the relative difference in innovation between some developing countries and the United States, which is the home of Silicon Valley. In the U.S. there is still no national contact tracing app. Instead individual states (such as North and South Dakota) have had develop their own. But at a national level, the rate of innovation has been painfully slow. In contrast, some developing countries have moved with amazing speed. One of the success stories has been Ethiopia. As Simon Marks described in an article on the Voice of America website, Ethiopian developers quickly created seven different apps to help with everything from contact tracing to supporting health care workers. What is clear is that the size of nation’s economy does not necessarily correspond to its ability to innovate and adapt. American exceptionalism aside, wealthy nations must overcome the hubris and sense of exceptionalism, which have hampered their response to the pandemic. When developed nations take an interest in the the innovations in places from Ethiopia to Thailand, their own response will improve.
A few years ago, I was in Hong Kong, Macau and Shenzhen. When I asked at a coffee shop in Hong Kong if I could pay with a credit card, the clerk said that they could do that. Would I mind waiting while they took the machine out from the cupboard? It would take just a minute to find the keys to the cupboard. At this point, I was embarrassed and ask them not to. But they wanted to help me, and insisted on hooking up the credit card machine for the foreigner. But credit cards felt antiquated in a world in people used WeChat to pay for their subway cards, get their groceries, and order deliveries. People never had touch a device to put in a PIN. When I came back, I realized how antiquated our entire payment architecture is. I think about this during the pandemic every time I go to a gas station or department store and have to first swipe a card, and then put in my PIN on a grungy pad. Of course this is the tip of the iceberg. Why do I still need to pay bills with a check in an age of Venmo and Paypal? In Australia checks have nearly disappeared as a payment form, and it has been more than a decade since most people used one. Five years ago I was talking with an Australian. She said that she was stunned when she moved to the U.S. and people still wanted checks. And why do forms in the US still ask for my department’s fax number?
In Shenzhen I saw the sophisticated drones, electronic devices, and pristine infrastructure. Afterwards when I traveled to New York and saw the state of the airport, it felt like traveling twenty years back in time. In the United States, there is a sense of exceptionalism, which equates modernity and power with being American. But from Asia to Africa there are innovations, technologies and approaches that Western nations -particularly the United States and Britain- would benefit from adopting, particularly during this pandemic. It’s not that the developed/developing binary doesn’t isn’t useful in some circumstances. But in some respects it can conceal more than it reveals.
Image of globe on light, McGill University. Photo by Smallman
In episode three of my podcast, “Dispatch 7: Global Trends on all seven continents” I interviewed my honors thesis student Samantha G. Alarcon Basurto about anemia in Peru. You can find the podcast on different platforms (including Apple podcasts), as well as on Anchor here:
Food market in Taiwan. Note the plastic partitions separating customers. Photo taken by Isabella Mori in May 2020.
Like many people, I’ve been struck by the parallels between the current COVID-19 pandemic and the 1918 pandemic. In 1918 many media outlets in Europe and the United States did not initially give the outbreak adequate coverage, because they were censored during the war, or did not want to reveal their nation’s weaknesses. In the United States and Brazil now, populist leaders are dismissive of the news and data on COVID-19, because it reveals their failures. For this reason, their followers tend to view all COVID-19 information through the lens of partisan politics. Indeed, President Bolsonaro of Brazil has called his followers to storm hospitals to take photos and videos to show whether COVID-19 patients are truly filling hospital beds, as the hospitals and state leaders claim. Such denial has caused painful climbs in COVID-19 deaths in both Brazil and the United States. …